
A medtech company arrives in the NHS with what appears to be a breakthrough.
The procedure is less invasive. The device is clever. Recovery may be faster. The surgeon can see the clinical logic. The patient’s story is persuasive. A medical society may even believe the technique represents the future of care.
Then the hospital finance team asks the question that decides adoption:
what are we paid, and what does it actually cost us to do this?
That is where many surgical innovations meet NHS reality.
A procedure can be clinically attractive yet financially difficult. It can be safe, codable, and used by surgeons, yet still fall into an old payment category built around older operations, devices, and assumptions.
That is the NHS innovation trap:
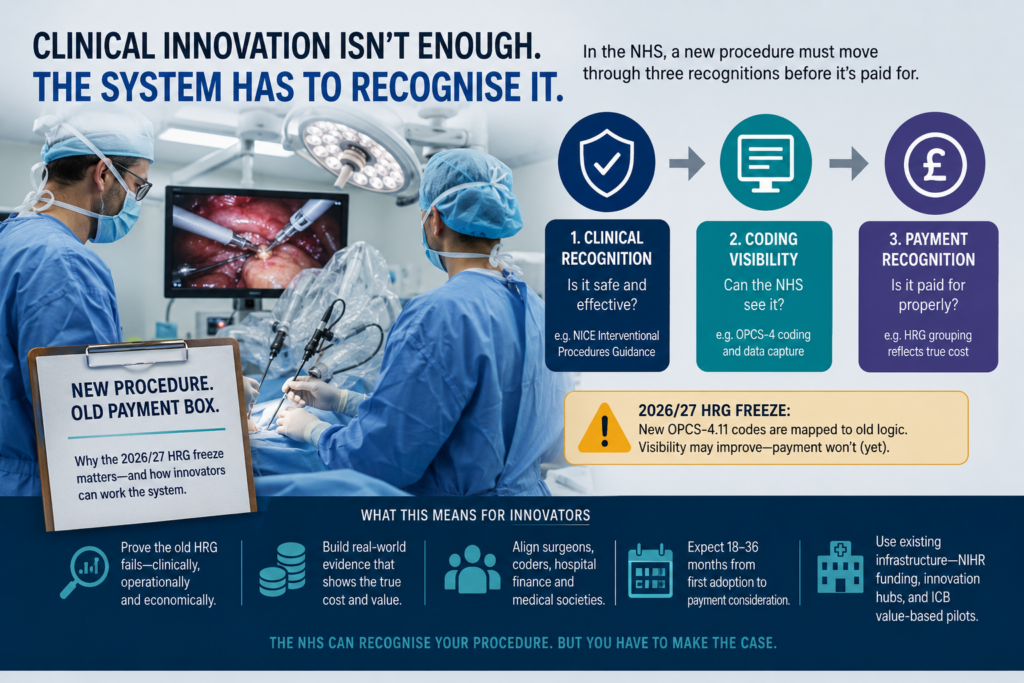
new procedure, old payment box.
For 2026/27, this problem has become more important because NHS England has effectively introduced a freeze in the new HRG design.
This is not a freeze of NHS payment overall. The 2026/27 NHS Payment Scheme is live. Hospitals are still being paid. Activity is still being processed. But NHS England has postponed the HRG4+ 2026/27 Local Payment Grouper and HRG design. Instead, new OPCS-4.11 procedure codes are being mapped back into OPCS-4.10-equivalent logic, so data can continue to be processed through the HRG4+ 2025/26 Local Payment Grouper. NHS England links this postponement to financial volatility concerns arising from the scale of change from OPCS-4.11 and the updated National Coding Standards.
That sounds technical.
It is not.
It is a strategic signal.
The NHS is saying, in effect:
coding may change, but payment will not automatically follow.
For companies introducing a new surgical procedure, implant, device-assisted intervention or operative technology, that distinction matters enormously. A procedure may become visible in coding. It may have a clearer administrative identity than before. It may even be performed in NHS hospitals. But if the payment grouper still treats it through older logic, the hospital may still be paid as if it had performed the older procedure.
In plain English:
the NHS may see the innovation before it pays for it properly.
That is why the 2026/27 HRG freeze matters.
Why the freeze was introduced
The freeze was introduced because NHS England was trying to avoid financial volatility.
Too much was changing at once.
OPCS-4.11 introduced new and revised procedure coding. National Coding Standards were updated. If NHS England had introduced a new HRG design at the same time, hospitals and commissioners could have seen unpredictable shifts in payment.
Some providers might suddenly gain.
Others might suddenly lose.
Commissioners might face unexpected cost movement.
Activity that used to fall into one payment group might move into another.
That is what financial volatility means.
In a health system under severe pressure, that matters. Payment architecture is not just a technical engine. It determines provider income, commissioner expenditure, service sustainability and financial risk.
So NHS England chose stability.
It allowed new procedure coding to move forward, but held back the new HRG architecture.
That is why this can reasonably be described as a 2026/27 HRG design freeze. Not a freeze of all payment, but a freeze of the new HRG grouper and design.
This is the key economic lesson:
The NHS has separated procedure visibility from payment recognition.
That is the heart of the story.
Procedure visibility: the first economic event
When we talk about visibility of a procedure, we do not mean marketing visibility, conference visibility or surgeon enthusiasm.
We mean something much more concrete:
can the NHS administrative system actually see that the procedure happened?
In England, that usually means OPCS-4 coding. OPCS-4 is the mandatory information standard used for clinical coding of hospital interventions and procedures undertaken by the NHS, and it supports analysis of healthcare data across the health service.
This is the first economic event in NHS reimbursement.
Until the NHS can code a procedure, the procedure barely exists for payment purposes.
If the procedure is not coded accurately, it becomes hidden inside older activity. It may be performed in theatre, discussed by surgeons, valued by patients and described in publications. But in the administrative data, it may look like something else.
That creates a chain reaction:
If the procedure is not coded, it is not visible.
If it is not visible, it cannot be counted.
If it cannot be counted, it cannot be costed.
If it cannot be costed, no one can prove the HRG payment is wrong.
This is why visibility matters.
A new surgical procedure does not become reimbursable because surgeons like it. It becomes reimbursable when the NHS can identify it, count it, cost it, compare it and decide whether the current payment structure is adequate.
That is why a medtech company, surgeon, physician or medical society must treat coding as part of the science of adoption, not as an administrative afterthought.
The 2026/27 freeze makes this even more important. OPCS-4.11 may improve coding visibility, but if activity is mapped back to OPCS-4.10-equivalent logic and processed through the 2025/26 grouper, visibility does not automatically translate into payment recognition.
Visibility is the beginning of reimbursement strategy.
It is not the end.
HRGs are not innovation badges
Many companies enter the NHS with the wrong question:
“How do we get a new HRG?”
That sounds logical. But it is usually the wrong starting point.
A Healthcare Resource Group is not a badge of innovation. It is not a prize for being robotic, digital, minimally invasive, implantable, AI-enabled or scientifically elegant.
An HRG is a payment currency. It groups activity that is expected to be clinically similar and to consume broadly similar NHS resources.
The NHS does not create or refine HRGs simply because a technology is impressive. It changes payment architecture when evidence shows that the existing architecture no longer describes reality.
So the better question is not:
“Can we get a new HRG?”
It is:
“Can we prove that the current HRG fails?”
That is the heart of surgical reimbursement strategy in England.
The three recognitions companies confuse
The 2026/27 HRG freeze exposes one of the most common mistakes in NHS market access.
Companies often assume that if a procedure is clinically accepted and coded, reimbursement will follow.
It does not work like that.
There are three different forms of recognition.
They are connected, but they are not the same.
1. Clinical governance recognition
This asks:
can the procedure be used safely and responsibly?
For a genuinely new surgical or invasive procedure, this may involve NICE Interventional Procedures Guidance. NICE’s interventional procedures programme evaluates whether procedures are safe enough and work well enough for NHS use. NICE may recommend standard arrangements, special arrangements, research-only use, or advise against use, depending on the evidence.
This matters enormously. It tells hospitals whether they can introduce the procedure and under what governance conditions.
But it is not payment.
A procedure can be allowed and still not be properly funded.
2. Coding visibility
This asks:
can the NHS record what happened?
This is OPCS territory.
If the procedure cannot be coded accurately, it becomes invisible in NHS data. If it is miscoded, it may be assigned to an older procedure category. If it disappears, the evidence chain breaks.
This is why OPCS visibility is the true gateway to future reimbursement reform.
But coding is still not payment.
A procedure can be coded and still be financially unattractive.
3. Payment recognition
This asks:
is the procedure paid differently because its cost, complexity or resource use is different?
This is the hardest stage.
The NHS may recognise the procedure clinically. OPCS may describe it administratively. But the HRG may still group it into an older payment category.
That is exactly why the 2026/27 freeze matters. OPCS-4.11 may provide updated coding visibility, but if activity is mapped back into OPCS-4.10-equivalent logic and processed through the 2025/26 grouper, the payment system may not yet recognise the innovation economically.
In simple terms:
NICE may allow it.
OPCS may describe it.
The HRG may still underpay it.
That is the problem.
The commercial barrier nobody wants to discuss
Imagine a new surgical procedure using a £6,000 device.
It reduces length of stay.
It may avoid later revision surgery.
It improves recovery.
Surgeons like it.
Patients may benefit.
But the hospital is paid through an HRG designed around the older, cheaper procedure.
The result is obvious.
The procedure may be clinically better, but financially worse for the provider.
That is where adoption slows.
The surgeon sees value.
The patient sees hope.
The company sees innovation.
The hospital sees a deficit.
This is not because the NHS is anti-innovation.
It is not because clinicians lack imagination.
It is not because the evidence is irrelevant.
It is because the provider cannot afford to lose money every time the procedure is performed.
That is the brutal truth of NHS surgical innovation:
Clinical value is insufficient if the provider’s economics fail.
The budget-silo problem: when the NHS saves money, but the hospital does not
Some innovations create a more subtle problem.
They save money for the NHS, but not necessarily for the organisation that has to implement them.
A useful example is the surgical glove change intervention during caesarean birth. A 2026 study based on real-world maternity service data from Royal United Hospitals Bath NHS Foundation Trust estimated that routine glove change could generate £339,654 in savings over five years at that trust. But most of those savings were not simply theatre savings. They came from fewer community midwife postnatal visits, reduced hospital readmissions and fewer GP appointments linked to infection-related care. Across NHS England, the same type of intervention was estimated to have potential savings of £45.1 million over five years.
This is exactly the economic problem surgical innovators must understand.
The value may be real, but the savings may sit in different budgets.
The theatre team changes practice.
The maternity unit implements the intervention.
The community midwife workload falls.
GP appointments are avoided.
Readmissions are reduced.
The system saves money.
But unless the business case shows who pays, who saves and how the benefit is captured, the adopting provider may not see the full financial reward.
That is the budget-silo problem.
For medtech, this is critical. Many surgical technologies do not create value inside the procedure alone. They create value downstream: fewer infections, fewer revisions, fewer readmissions, shorter stays, fewer outpatient visits, faster recovery, less community support, better function and fewer complications.
Those are real economic benefits.
But the NHS needs them translated into a budget map.
Which organisation pays?
Which organisation saves?
Which part of the pathway changes?
Which budget line moves?
Can the savings be captured locally, or only system-wide?
Without this, even a cost-saving innovation can struggle.
How a new procedure is really created in the NHS
A new procedure is not created by a company alone.
It is created by a coalition.
A medtech company may invent the device or platform.
A surgeon or physician may define the clinical use case.
A medical society may validate the unmet need and procedural standards.
A hospital may generate the early data.
Coders translate the procedure into administrative language.
Health economists translate it into resource consequences.
NICE and governance teams decide how it can be used responsibly.
Commissioners and finance teams decide whether the system can afford it.
This is why the best NHS innovation strategies are not sales campaigns.
They are category-building exercises.
The question is not simply:
“Can we sell this technology?”
The question is:
“Can we create a recognised clinical activity that the NHS can safely govern, accurately code, reliably measure and eventually pay for?”
That is how procedures become real in the NHS.
The role of medtech companies
For a medtech company, the first task is not to demand reimbursement.
It is to define the procedure with surgical and economic precision.
That means answering:
Which patients?
Which anatomical indication?
Which procedural steps?
Which comparator?
Which existing OPCS codes?
Which HRG does it currently group to?
What is the device cost?
What theatre time is required?
What length of stay changes?
What complications are avoided?
What revisions or readmissions are reduced?
Which provider pays?
Which part of the system saves?
A company that cannot answer those questions is not ready for serious NHS adoption.
The medtech company must move from product claim to procedure claim.
Not:
“Our device is innovative.”
But:
“This procedure changes the patient pathway in these defined patients, creates these resource consequences, and exposes a mismatch in the current HRG payment.”
That is the NHS language.
The role of surgeons and physicians
For surgeons and physicians, the task is different.
They are often the ones who can see the clinical gap first.
They know where current procedures fail, where patients are poorly served, where revision burden is high, where anatomy is difficult, where complications are predictable and where existing techniques are no longer good enough.
But clinical enthusiasm is not enough.
A surgeon who wants to introduce a new procedure must help define:
the patient-selection criteria,
the comparator procedure,
the technical steps,
the learning curve,
the safety risks,
the expected outcomes,
the audit dataset,
the complications to track,
the follow-up pathway,
and the resource consequences.
This turns clinical intuition into a procedure.
A physician or surgeon can say:
“This is not simply a new device. This is a different clinical act, in a defined patient group, with different risks, costs and outcomes.”
That statement is the beginning of reimbursement logic.
The role of medical societies
Medical societies can be decisive because they can turn scattered clinical enthusiasm into disciplined procedural practice.
A good example is hip fracture care. The fragility hip fracture Best Practice Tariff was developed around defined clinical characteristics of best practice, including prompt surgery and appropriate involvement of geriatric medicine. The tariff logic was linked to clinical standards and the National Hip Fracture Database, with eligibility requiring specific criteria such as timely surgery, joint orthopaedic-geriatric care and structured assessment.
This is important because it shows what professional structure can do.
The payment system did not reward vague “better care”. It rewarded a defined pathway.
The clinical community helped define what good care meant. The audit infrastructure measured whether hospitals delivered it. The payment mechanism then incentivised the behaviour.
That is the model surgical innovators should study.
A medical society can help define:
which patients should be eligible,
which centres should perform the procedure,
which training standards are required,
which registry variables should be collected,
which outcomes matter,
which complications should be audited,
which existing procedures are the comparator,
and when the new procedure should or should not be used.
This matters because payment systems do not like uncontrolled indication creep.
If a new procedure is positioned too broadly, payers become nervous. If it is positioned too vaguely, coders struggle. If it lacks standards, hospitals hesitate.
A medical society can create discipline.
That discipline strengthens the reimbursement case.
The best society-led innovation work says:
“This procedure is not for everyone. It is for this defined subgroup, in these circumstances, performed by trained teams, measured through these outcomes, and compared against this standard of care.”
That is exactly the type of clinical structure that payment systems can eventually recognise.
Why the 2026/27 freeze changes strategy
The freeze changes the strategic starting point.
Before, a company might have hoped that new procedure coding and payment design would evolve together.
In 2026/27, NHS England has made clear that this will not necessarily happen.
The payment year has moved on, but the underlying HRG architecture has been held back.
That means innovators must model conservatively.
Do not assume:
new code = new HRG = new payment.
Assume:
new code = old payment until proven otherwise.
That is the safer and more realistic NHS strategy.
For a company, surgeon or medical society, this means the reimbursement plan must be built around evidence of payment failure.
You need to show:
where the procedure currently groups,
what the hospital is paid,
what the procedure actually costs,
why the current HRG is inadequate,
what patient subgroup is different,
what resource use is different,
what costs are avoided,
what outcomes improve,
and what real-world evidence will prove it.
That is how you work the system
The NHS surgical innovation playbook
A company entering the NHS with a new surgical procedure should not begin with a sales deck.
It should build a reimbursement evidence pack.
1. Define the procedure, not the product
The NHS does not reimburse adjectives.
It reimburses recognised clinical activity.
So do not begin with:
“a revolutionary surgical platform.”
Begin with:
which patient, which anatomy, which technique, which device, which comparator, which setting, which operator, which length of stay, which complications, which follow-up pathway and which budget.
If the procedure cannot be described precisely, it cannot be coded precisely.
If it cannot be coded precisely, it cannot be reimbursed intelligently.
2. Establish the governance position
If the procedure is genuinely new or being used in a new way, determine whether NICE Interventional Procedures Guidance is needed.
A favourable NICE position does not guarantee payment, but it gives hospitals confidence that the procedure can be introduced responsibly.
Without governance clarity, even interested clinicians may struggle to persuade their organisation to adopt.
3. Secure OPCS visibility
This is the administrative gateway.
Identify the relevant OPCS codes. Check whether existing codes genuinely describe the new procedure or simply hide it inside an older category. Determine whether supplementary coding is needed. Make sure hospital coders can record the activity consistently.
This is not bureaucracy.
This is commercial survival.
A miscoded procedure disappears into the system.
A disappeared procedure cannot generate evidence.
A procedure without evidence cannot change payment.
4. Model where it groups
Once the procedure is coded, determine where it groups under current HRG logic.
For 2026/27, companies must be especially conservative because OPCS-4.11 codes may be mapped back into OPCS-4.10-equivalent logic and processed through the 2025/26 grouper.
So the question becomes:
which old payment box does the new procedure fall into?
That is the number every company needs.
5. Quantify the provider funding gap
This is the heart of the business case.
What is the hospital paid?
What does the procedure actually cost?
If there is a gap, explain it precisely.
Is it driven by:
device cost,
theatre time,
imaging,
navigation,
robotic support,
consumables,
training,
the learning curve,
more complex patients,
or follow-up requirements?
Do not say:
“The procedure is innovative.”
Say:
“The current HRG pays £X. The procedure costs £Y. The gap is driven by these specific resource elements.”
That is the language the NHS understands.
6. Build a local NHS business case
Most NHS adoption starts locally.
The first adopter may be a specialist centre, teaching hospital, surgical network, Integrated Care Board pathway or research-active NHS trust.
The local business case must answer one practical question:
why should this organisation adopt the procedure now, despite uncertainty in national payment?
That may involve:
research funding,
innovation funding,
local payment adjustment,
specialised commissioning logic,
pathway redesign,
shared savings across an Integrated Care Board,
or a controlled real-world evidence programme.
Do not write the business case for “the NHS”.
Write it for the organisation that has to pay, implement and defend the decision.
7. Generate evidence that the old payment box fails
This is the decisive move.
The company needs real NHS data:
coded activity,
case-level costing,
device cost,
theatre time,
length of stay,
complications,
readmissions,
revision rates,
follow-up burden,
patient outcomes,
and comparative pathway economics.
Only then can the innovator credibly say:
the existing HRG no longer describes this procedure.
That is when payment reform becomes possible.
What a credible evidence package looks like
“Generate evidence” is too vague.
For an HRG challenge, the evidence package must be designed around payment failure.
The most persuasive package usually includes five layers.
1. Activity visibility
Show that the procedure is being coded consistently across sites.
This means:
OPCS code use,
diagnosis codes,
patient subgroup,
provider site,
case volume,
day-case versus inpatient status,
and extraction from hospital datasets.
Without activity visibility, there is no reimbursement argument.
2. Provider cost evidence
Show what the hospital actually spends.
This should include:
device or implant cost,
consumables,
theatre time,
staff mix,
anaesthesia time,
imaging or navigation costs,
ward stay,
critical care use if relevant,
follow-up appointments,
and revision or complication costs.
This is where the provider funding gap becomes visible.
3. Comparator evidence
Show what the old pathway costs.
The NHS must understand what the new procedure replaces.
The comparator may be:
open surgery,
standard laparoscopic surgery,
non-operative management,
repeat revision surgery,
long-term conservative care,
or another device-assisted pathway.
The comparator must be clinically credible. If surgeons reject the comparator, the economics will not survive.
4. Outcome evidence
Show what improves.
For surgical procedures, the most useful measures often include:
length of stay,
day-case conversion,
readmission rates at 30 and 90 days,
complication rates,
reoperation or revision rates,
infection rates,
return to function,
patient-reported outcome measures,
mortality where relevant,
pain, mobility or continence outcomes depending on specialty,
and resource use over 6, 12 and 24 months.
The time horizon depends on the claim.
If the claim is shorter stay, 30 to 90 days may be enough.
If the claim is fewer revisions, less degeneration, better continence or reduced long-term complications, 12 to 24 months is usually more credible.
5. Economic translation
Finally, translate outcomes into NHS economics.
Do not simply say outcomes improve.
Show:
which costs fall,
where savings occur,
whether savings are inside the hospital or elsewhere in the system,
whether the provider benefits,
whether the commissioner benefits,
whether the Integrated Care Board benefits,
and whether the HRG payment remains inadequate despite system value.
This is where the glove-change example is instructive. The intervention appears clinically and economically valuable, but the savings are distributed across different parts of the pathway. That is exactly why the business case must map costs and savings to the budget holder, not just to the theoretical NHS value.
How long this actually takes
This is the part many companies underestimate.
Creating payment recognition in England is rarely quick.
A realistic timeline is often:
0–6 months: procedure definition, NICE/guidance review, coding assessment and first NHS partner identification.
6–12 months: early adopter business case, governance approval, first cases and coding validation.
12–24 months: real-world evidence collection, provider cost analysis, outcome tracking and local pathway economics.
24–36 months: multi-site evidence, stronger health economic case, medical society support, NICE HealthTech or policy engagement, and early arguments for payment refinement.
For some procedures, this may be faster.
For complex implantable or surgical technologies, it may be slower.
The important point is expectation-setting. If a company expects national payment recognition in six months, it will become frustrated. If it understands that the NHS needs visible activity, local evidence and proof of payment failure, the strategy becomes more rational.
In England, the sequence is slow because the burden of proof is high.
But it is not mysterious.
The infrastructure that can help
The pathway is difficult, but not impossible.
There is infrastructure that can support innovators.
NIHR’s Invention for Innovation (i4i) programme is specifically aimed at medical devices, in vitro diagnostics and digital health technologies addressing health or social care needs. It supports collaborative research and development projects for technologies intended for NHS or social care use. NIHR’s Product Development Awards can support activities from R&D through to implementation of transformative technologies in health and care settings, with projects commonly lasting two to three years.
NIHR also states that it funds commercial and non-commercial research to accelerate innovation in therapeutics, medical devices, diagnostics and health technologies for use in the UK’s NHS or care environment.
NHS Supply Chain is also developing Value Based Procurement, explicitly shifting from cash-releasing savings alone toward value-based procurement that considers broader benefits and practical application across the NHS.
This matters because some procedures may never look attractive if assessed only on upfront device price.
They may become attractive when assessed through:
reduced complications,
shorter recovery,
fewer readmissions,
reduced pathway cost,
lower revision burden,
better use of theatre capacity,
or improved long-term patient outcomes.
That is exactly where value-based procurement, innovation funding, early adopter trusts, research-active hospitals and Integrated Care Board pathway redesign can help.
These mechanisms do not remove the need for evidence.
They create places where evidence can be generated.
How to create a new procedure category
This is the deeper point.
A new procedure category is not created by saying, “we need reimbursement”.
It is created by proving that existing clinical and payment categories are no longer sufficient.
That requires four layers of evidence.
First, clinical distinctiveness.
The procedure must be meaningfully different from existing practice. Not just a new instrument, but a different clinical act, in a defined patient group, with different risks, outcomes or resource consequences.
Second, coding distinctiveness.
The procedure must be visible in data. If existing OPCS codes hide it, the innovation has no administrative identity.
Third, economic distinctiveness.
The procedure must have a cost or resource profile that differs from the existing HRG. That may mean higher device cost, different theatre time, shorter stay, fewer complications, fewer readmissions, reduced revision burden or a shift from inpatient to day-case care.
Fourth, policy distinctiveness.
The procedure must matter to the NHS. It must solve a problem the system recognises: bed capacity, waiting lists, avoidable complications, expensive revisions, poor outcomes, workforce pressure, unmet need or inequality of access.
Only when those four layers align can a medtech company, surgeon or medical society credibly argue:
This is not merely a new product inside an old procedure. This is a new procedure category that the NHS should recognise.
Why England is different from Germany
This is where many European market access strategies go wrong.
Germany has a more visible hospital innovation bridge. A new hospital technology may move through OPS coding, NUB applications, temporary local negotiation and eventual DRG or Zusatzentgelt integration.
England is different.
England does not usually offer the same visible interim payment bridge for new surgical procedures. It asks colder questions:
Can we see it?
Can we code it?
Can we govern it?
Can we group it?
Can the provider afford it?
Can the innovator prove the old payment is wrong?
This does not make England anti-innovation.
It makes England evidence-heavy and payment-conservative.
The NHS may recognise clinical innovation before it recognises financial innovation.
That is the point.
What every surgical innovator needs before entering the NHS
A serious NHS market entry strategy should include seven documents.
1. Procedure Definition Paper
What exactly is the procedure, for which patients, in which setting and against which comparator?
2. NICE Governance Memo
Does the procedure need NICE Interventional Procedures Guidance? If guidance exists, what does it say?
3. OPCS Coding Strategy
How will the procedure be coded? Does existing coding capture it properly or hide it inside older activity?
4. HRG Impact Model
Which HRG does the procedure currently group to, and what payment does the provider receive?
5. Provider Economics Model
What does the procedure actually cost the hospital, including device, theatre time, staffing, consumables, stay and follow-up?
6. Local NHS Business Case
Why should an early NHS adopter introduce this procedure despite uncertainty in national payment?
7. Real-World Evidence Plan
What data will prove that the current payment structure fails?
This is how to work the NHS.
Not by asking the system to admire the innovation, but by proving that the old payment category cannot contain it.
Final lesson
The 2026/27 HRG freeze is a technical event with a strategic message.
It shows that NHS England is willing to let coding evolve while keeping payment architecture stable. That is rational. It protects the system from financial volatility.
But it also creates a challenge for innovators.
The NHS may see the procedure before it pays for it properly.
In England, a new surgical procedure must become:
clinically acceptable,
codable,
measurable,
economically defensible,
locally adoptable,
and professionally legitimate
before national payment recognition becomes realistic.
The NHS does not pay for novelty.
It pays for recognised activity.
The genius move is not to demand a new HRG.
The genius move is to prove that the old payment box no longer fits.