
Receiving FDA clearance or approval is one of the defining moments in a medical technology company’s life.
It is also the point at which many companies discover that regulatory success and commercial access are not the same thing.
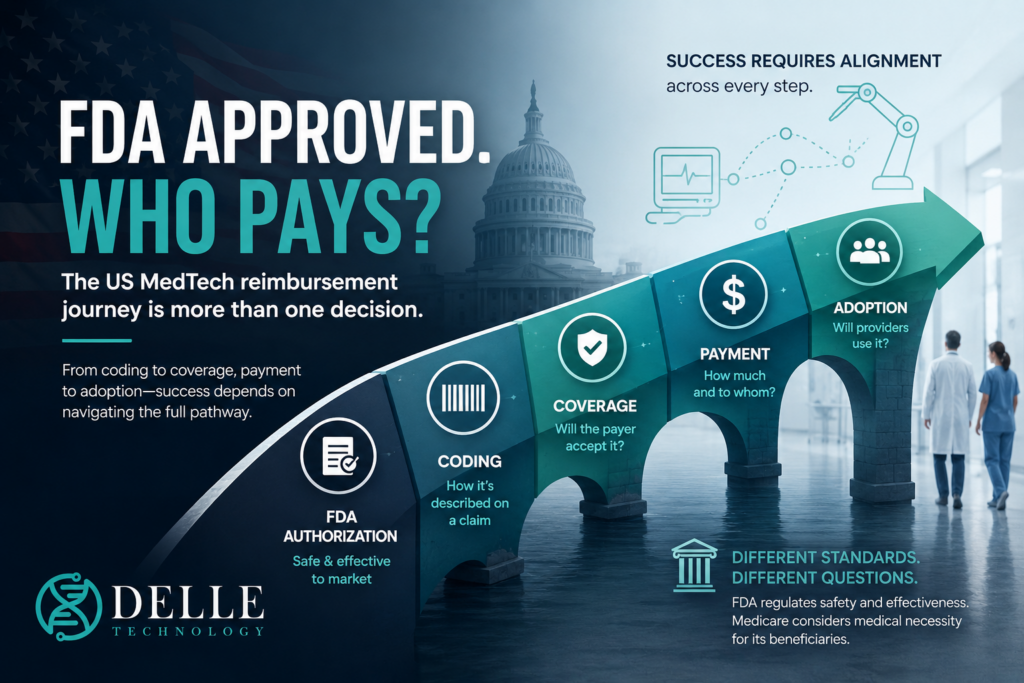
FDA authorisation allows a device to be marketed for its authorised intended use. It does not create a billing code, establish Medicare coverage, determine payment or compel a hospital to buy the product.
The US reimbursement pathway is therefore not one decision. It is a chain of decisions:
FDA authorisation → benefit-category fit → coding → coverage → payment → hospital adoption → patient access
A weakness anywhere in that chain can prevent a clinically valuable technology from reaching routine care.
This guide explains how to build a US MedTech reimbursement strategy, what each organisation decides and what a company should do at every stage.
Step 1: Define the service not merely the device

The first mistake is to begin by asking:
What reimbursement code does our device need?
The better question is:
What clinical service is being delivered, where is it delivered, who performs it, who purchases the technology and who submits the claim?
US payment systems generally reimburse healthcare services, episodes of care, procedures, professional work, equipment or supplies. They do not necessarily reimburse a product simply because the FDA has authorised it.
Begin by mapping:
- the patient population;
- the present treatment pathway;
- the new pathway created by the technology;
- the healthcare professional using it;
- the organisation purchasing it;
- the site of care;
- the claimant;
- the incremental resources;
- the clinical and economic benefits.
The site of care is especially important. A technology can have different reimbursement consequences when used in an inpatient hospital, hospital outpatient department, ambulatory surgical centre, physician office, laboratory or patient’s home.
A device may be separately payable in one setting and included within a bundled payment in another.
What to do
Produce a one-page care-pathway map before applying for a new code or approaching a payer.
The map should show who performs the service, who buys the product, which organisation bills the payer and where the financial benefit occurs.
Step 2: Understand what FDA authorisation does—and does not do
The FDA regulates whether a medical device may legally be marketed in the United States.
Routes include:
- 510(k) clearance;
- De Novo classification;
- Premarket Approval;
- exemptions for certain lower-risk devices.
The appropriate route depends on the product’s risk, novelty and regulatory history. The FDA’s official device pathways are explained through its device-advice resources and classification materials.
Official FDA device pathways:
How to Study and Market Your Device
FDA authorisation is necessary for most technologies, but Medicare applies a different legal test.
CMS explains that Medicare coverage is limited to items and services that fall within a Medicare benefit category and are reasonable and necessary for diagnosis or treatment.
CMS has also stated that FDA clearance or approval alone does not entitle a technology to Medicare coverage.
This means the FDA and CMS may review some of the same studies but ask different questions.
FDA may focus on whether the technology is sufficiently safe and effective for marketing. CMS may additionally ask:
- Does the evidence apply to Medicare-aged patients?
- Are important comorbidities represented?
- Does the technology change patient management?
- Is the benefit clinically meaningful?
- Is the outcome durable?
- Will the technology work outside specialist centres?
- What provider or facility qualifications are necessary?
What to do
Create a payer-evidence plan alongside the FDA clinical plan.
Do not assume that endpoints selected for regulatory authorisation will automatically support Medicare or commercial coverage.
Step 3: Establish Medicare benefit-category fit
Before Medicare decides whether a technology is reasonable and necessary, there must generally be a statutory basis under which it can be covered.
Possible benefit categories include:
- inpatient hospital services;
- outpatient hospital services;
- physician services;
- diagnostic tests;
- durable medical equipment;
- prosthetic devices;
- certain home-health services;
- other specifically defined Medicare benefits.
This issue is frequently underestimated.
Traditional implants and surgical instruments may fit established pathways. Stand-alone software, digital therapeutics, remote platforms and algorithmic services may be harder to place within existing benefit structures.
The official CMS guide is the best starting point. It covers Medicare Part A and Part B Fee-for-Service and treats coding, coverage and payment as related but separate processes.
Official CMS guide:
CMS Guide for Medical Technology Companies and Other Interested Parties
What to do
Document:
- the proposed Medicare benefit category;
- why the technology or service fits it;
- the responsible provider or supplier;
- any enrolment or certification requirements;
- whether the technology is used inside another covered service.
A strong clinical case cannot compensate for the absence of a viable benefit category.
Step 4: Determine whether existing codes are sufficient
Coding describes what happened during care. It does not, by itself, establish coverage or payment.
Relevant systems include:
CPT
The American Medical Association maintains CPT codes for medical services and procedures performed by physicians and other qualified healthcare professionals.
Category I codes generally describe established services.
Category III codes provide temporary reporting mechanisms for emerging technologies, services and procedures. They can support consistent claims reporting and utilisation tracking, but do not guarantee payment.
AMA coding application information:
CPT code change applications
HCPCS Level II
CMS maintains HCPCS Level II codes, commonly used for supplies, equipment, products and services not described fully through CPT.
Official CMS coding overview:
CMS Medical Technology Guide: Coding
ICD-10-PCS
ICD-10-PCS describes procedures performed during inpatient hospital admissions. A new procedure code may improve visibility but does not itself guarantee a different MS-DRG or higher payment.
ICD-10-CM
Diagnosis codes identify the condition being treated and may influence medical necessity and payment classification.
PLA codes
Proprietary Laboratory Analyses codes can identify certain proprietary diagnostic tests. Test-specific coding remains separate from payer coverage and payment policy.
What to do
Conduct a coding audit:
- Identify all current diagnosis, procedure, professional and product codes.
- Test whether they accurately describe the new service.
- Determine whether the technology is visible or hidden within a broader claim.
- Evaluate whether an unlisted code is workable during launch.
- Apply for a new code only when the existing systems are materially inadequate.
A new code application can take time and must be supported by a clear description of the service—not merely the novelty of the product.
Step 5: Build a coverage strategy
Coverage determines whether a payer accepts the service for a defined patient, indication and care setting.
For Medicare Fee-for-Service, coverage may arise through:
- a National Coverage Determination;
- a Local Coverage Determination;
- case-by-case claims adjudication;
- Coverage with Evidence Development;
- an emerging-technology pathway.
National Coverage Determinations
CMS makes NCDs through an evidence-based process with opportunities for public participation. The process may involve an external technology assessment or MEDCAC advice.
Current CMS coverage-process page:
Medicare Coverage Determination Process
CMS’s formal NCD notice also explains that the process begins after a complete formal request has been accepted. Preliminary discussions and evidence preparation may occur before the statutory timetable begins.
Local Coverage Determinations
Where no NCD exists, Medicare Administrative Contractors may establish local policies.
This can allow a company to launch through selected regions or specialist centres, but it may also create geographic variation.
Commercial coverage
Commercial insurers are not automatically bound by Medicare decisions.
They may apply their own:
- evidence standards;
- medical-necessity policies;
- prior-authorisation rules;
- network restrictions;
- investigational exclusions;
- payment contracts.
What to do
Create a payer map showing:
- whether an NCD exists;
- relevant LCDs;
- current commercial policies;
- evidence gaps;
- target patient criteria;
- prior-authorisation requirements;
- the most realistic initial coverage route.
Do not seek an NCD merely because national coverage sounds desirable. A local or account-based launch may sometimes be more practical.
Step 6: Decide how the provider will be paid
Coverage does not necessarily mean separate payment.
CMS acknowledges that a covered item may still be included in a bundled payment and that coding or payment questions may fall outside an NCD.
The payment route depends on the setting.
Inpatient hospitals
Medicare pays most acute inpatient admissions through MS-DRGs.
The hospital receives a prospective payment that must cover the whole admission, including the device, staff, operating theatre, imaging, ward care and complications.
A new technology can therefore improve outcomes while worsening the hospital’s financial position.
Qualifying technologies may apply for a New Technology Add-on Payment.
Official CMS NTAP page:
New Medical Services and New Technologies
NTAP is temporary and partial. It should be treated as a bridge into the ordinary MS-DRG system, not a permanent business model.
Hospital outpatient departments
Hospital outpatient services are generally paid under OPPS through Ambulatory Payment Classifications.
New technologies may be:
- packaged into an existing APC;
- assigned to a New Technology APC;
- eligible for temporary device pass-through payment.
Official CMS pass-through and New Technology APC page:
Pass-Through Payment Status and New Technology APC
Physician services
Professional work may be paid through the Medicare Physician Fee Schedule.
The company must determine whether the technology creates:
- new physician work;
- interpretation;
- monitoring;
- reporting;
- technical and professional components;
- no separately billable professional service.
What to do
Build a provider-level financial model for every relevant site of care.
It should show:
- current reimbursement;
- reimbursement after introduction;
- device acquisition cost;
- additional staffing or infrastructure;
- avoided resources;
- expected margin;
- the position after temporary payment expires.
The most important calculation is often not the payer’s total saving. It is the adopting provider’s incremental margin.
Step 7: Prepare for hospital value analysis
Hospitals do not adopt technologies solely because a code or coverage policy exists.
A hospital may require review by:
- clinicians;
- procurement;
- finance;
- value-analysis committees;
- IT;
- cybersecurity;
- legal and compliance;
- biomedical engineering;
- service-line management.
The decision may depend on:
- comparative clinical benefit;
- acquisition cost;
- budget impact;
- reimbursement;
- staffing;
- training;
- workflow;
- interoperability;
- procedure time;
- length of stay;
- complications;
- capacity;
- downstream testing.
What to do
Prepare a hospital value dossier containing:
- the clinical problem;
- current pathway;
- proposed pathway;
- comparative evidence;
- coding and payment map;
- budget-impact model;
- implementation plan;
- training requirements;
- cybersecurity and integration information;
- real-world data plan.
Present value from the hospital’s perspective, not merely the payer’s.
A technology can save the health system money while creating a financial loss for the organisation expected to buy it.
Step 8: Plan temporary and long-term reimbursement separately
Temporary mechanisms can accelerate early adoption, but they eventually expire.
Examples include:
- Category III CPT codes;
- NTAP;
- outpatient pass-through payment;
- Coverage with Evidence Development;
- emerging-technology programmes.
A company must understand what happens afterwards.
Questions include:
- Will utilisation data support a permanent code?
- Will costs enter DRG or APC calculations?
- Will evidence support unrestricted coverage?
- Can the hospital continue after supplemental payment ends?
- Will commercial contracts need renegotiation?
What to do
Develop a transition plan before the temporary pathway begins.
The plan should state:
- the evidence to be collected;
- the timetable;
- the permanent coding objective;
- the payment objective;
- the post-transition hospital economics.
Step 9: Treat emerging pathways carefully
CMS finalised the Transitional Coverage for Emerging Technologies pathway in August 2024 for selected Breakthrough Devices.
Official TCET notice:
Final Notice—Transitional Coverage for Emerging Technologies
In April 2026, CMS and FDA announced the proposed RAPID pathway and said TCET would be paused for new candidates while RAPID was developed. CMS also said RAPID would take effect after a final procedural notice.
Official RAPID announcement:
CMS and FDA Announce RAPID Coverage Pathway
The practical conclusion is that companies should monitor RAPID, but should not yet assume that it provides an automatic or operational route to immediate coverage.
Step 10: Design evidence for every decision-maker
One regulatory study rarely answers all market-access questions.
The evidence programme should address four audiences.
FDA needs safety, effectiveness and technical-performance evidence.
Payers need comparative benefit, population relevance, durability and impact on patient management.
Payment authorities may need cost data, resource utilisation, payment inadequacy and evidence of meaningful clinical improvement.
Hospitals need budget impact, implementation requirements, staffing, workflow and operational return.
What to do
Build an integrated evidence matrix listing:
- each decision-maker;
- the decision being made;
- the endpoint required;
- the evidence source;
- when the data will become available;
- who is responsible for collection.
This is the foundation of a genuine US MedTech reimbursement strategy.
The central lesson
FDA reimbursement is not a payment issued by the FDA.
It is the commercial and policy pathway that begins around FDA authorisation and continues through Medicare eligibility, coding, payer coverage, payment and provider adoption.
FDA authorisation permits market entry.
Benefit-category fit provides a possible legal basis for Medicare coverage.
Coding describes the service.
Coverage determines when a payer accepts it.
Payment determines whether delivery is financially viable.
Hospital adoption determines whether the technology reaches patients.
The best time to develop the reimbursement strategy is not after FDA authorisation.
It is while the clinical and regulatory programme is still being designed.
References and further reading
- Centers for Medicare & Medicaid Services. CMS Guide for Medical Technology Companies and Other Interested Parties. Updated 10 March 2026.
https://www.cms.gov/medicare/coding-billing/guide-medical-technology-companies-other-interested-parties - Centers for Medicare & Medicaid Services. Medicare Coverage Determination Process. Updated 12 March 2026.
https://www.cms.gov/medicare/coverage/determination-process - Centers for Medicare & Medicaid Services. Medicare Program: Revised Process for Making National Coverage Determinations. Federal Register. 2013;78:48164–48169.
https://www.govinfo.gov/content/pkg/FR-2013-08-07/pdf/2013-19060.pdf - Centers for Medicare & Medicaid Services. Final Notice—Transitional Coverage for Emerging Technologies. 7 August 2024.
https://www.cms.gov/newsroom/fact-sheets/final-notice-transitional-coverage-emerging-technologies-cms-3421-fn - Centers for Medicare & Medicaid Services and US Food and Drug Administration. CMS and FDA Announce RAPID Coverage Pathway. 23 April 2026.
https://www.cms.gov/newsroom/press-releases/cms-fda-announce-rapid-coverage-pathway-accelerate-patient-access-life-changing-medical-devices - Centers for Medicare & Medicaid Services. New Medical Services and New Technologies.
https://www.cms.gov/medicare/payment/prospective-payment-systems/acute-inpatient-pps/new-medical-services-and-new-technologies - Centers for Medicare & Medicaid Services. Pass-Through Payment Status and New Technology APC.
https://www.cms.gov/medicare/payment/prospective-payment-systems/hospital-outpatient/pass-through-payment-status-new-technology-ambulatory-payment-classification-apc - US Food and Drug Administration. How to Study and Market Your Device.
https://www.fda.gov/medical-devices/device-advice-comprehensive-regulatory-assistance/how-study-and-market-your-device - American Medical Association. CPT Appendix S: Taxonomy for Artificial Intelligence in Medical Services and Procedures. Updated 8 June 2026.
https://www.ama-assn.org/practice-management/cpt/cpt-appendix-s-taxonomy-artificial-intelligence-medical-services-procedures - Wu K, Wu E, Theodorou B, et al. Characterizing the clinical adoption of medical AI devices through US insurance claims. NEJM AI. 2024;1(1).
https://doi.org/10.1056/AIoa2300030 - Gupte T, Nitave T, Gobburu J. Regulatory landscape of accelerated approval pathways for medical devices in the United States and the European Union. Frontiers in Medical Technology. 2025;7:1586070.
https://doi.org/10.3389/fmedt.2025.1586070 - Sun E, Littenberg G. Reimbursement and regulatory landscape for artificial intelligence in medical technology. Gastrointestinal Endoscopy Clinics of North America. 2025;35(2).
https://www.giendo.theclinics.com/article/S1052-5157(24)00111-9/abstract
This format gives you real, publisher or government links in both the body and reference list, uses FDA reimbursement as the primary keyword, and turns the piece into a practical guide rather than a descriptive essay.