
The Promise and the Paradox
The UK Government’s 10-Year Health Plan for England (2025–2035) presents itself as a blueprint for a modernised NHS—one that is digitally enabled, outcomes-measured, genomically informed, and operationally productive. It offers a seductive narrative: faster diagnostics, AI-supported clinical decision-making, precision medicine, regional innovation zones, and a payment system redesigned around bundles, prevention, and “best-practice tariffs.”
But beneath the rhetoric lies a structural paradox familiar to health-systems researchers: ambition without capacity can generate inertia, not innovation.
In health economics, this is the “implementation friction” that occurs when regulatory expansion outpaces analytical throughput, workforce capability, capital investment, or data infrastructure. The UK is now entering that zone of tension.
The Plan’s expanded remit for NICE, the shift toward productivity-linked tariffs, the acceleration of digital pathways, and the decentralisation of commissioning power to Integrated Care Systems (ICSs) represent profound changes to the reimbursement architecture. In theory, they should align incentives, promote value, and accelerate diffusion of high-impact technologies. In practice, they risk creating the very conditions that slow innovation: approval backlogs, risk-averse commissioning, fragmented regional decision-making, and a widening gap between policy ambition and operational reality.
This commentary examines the health-system mechanics behind that tension.
We analyse how:
- expanded NICE mandates may convert a selective evaluation body into a national bottleneck;
- year-of-care bundled payments may induce insurance-style behaviours in ICSs;
- insourcing and elective recovery programmes attempt to solve capacity shortfalls without addressing structural deficits;
- digital-first pathways risk widening inequalities; and
- regionalisation could quietly erode the founding principle of universality.
The central insight is this: the NHS is being redesigned around concepts—productivity, digitalisation, genomic precision—that require capital, data architecture, and workforce elasticity that the current system does not possess. Without major investment in analytic capacity, clinical labour, estates, and informatics, the reforms may reshape the NHS not into a more innovative system—but into a more fragmented, slower, and more unequal one.
The years to 2035 will determine whether technology becomes a catalyst for renewal or a multiplier of system strain. The question is no longer whether the NHS should transform, but whether the foundations needed for that transformation truly exist.
NICE Under Pressure: Accelerator or Bottleneck?
NICE (link: https://www.nice.org.uk/) is being reshaped into a powerful central authority for:
NICE is being repositioned as the central gatekeeper for England’s innovation ecosystem—responsible not only for medicines, but for the full spectrum of modern health technologies: diagnostics, medical devices, AI-driven decision-support tools, digital therapeutics, genomic assays, and the systematic decommissioning of obsolete interventions.
This is a profound shift in institutional purpose.
NICE’s original architecture was built for selective, high-value appraisal, not for industrial-scale, rapid-cycle evaluation. Its processes—deep evidence synthesis, model critique, expert committee deliberation, and stakeholder consultation—reflect the traditions of classical HTA. They are scientifically rigorous, but structurally slow.
The Scientific and Operational Risks of the New Mandate
- Evaluation Volume Outpacing Analytical Capacity
AI, digital health, and point-of-care diagnostics generate high-frequency iteration cycles and continuous software updates.
Unlike pharmaceuticals, these technologies do not follow a linear, finite evidence trajectory.
Evaluating them at scale requires:- new statistical frameworks for adaptive algorithms,
- validation methodologies for real-time model drift,
- continuous real-world performance auditing.
NICE does not yet have the operational machinery or workforce bandwidth for this level of throughput.
- Delays to Adoption of High-Value Technologies
Under the 10-Year Plan, more categories of technology are required to undergo NICE appraisal before NHS commissioning.
This creates a single point of failure.
If appraisal pipelines grow faster than reviewer capacity, turnaround times will lengthen—directly contradicting the government’s ambition for rapid diffusion of innovation. - Shift from Clinical Evidence to Fiscal Gatekeeping
When NICE becomes the arbiter of affordability as well as evidence, economic pressure risks overshadowing clinical nuance.
With constrained NHS budgets, committees may feel compelled to apply stricter interpretations of cost-effectiveness thresholds or adopt conservative modelling assumptions that suppress value estimates for novel diagnostics, genomics, and AI tools. - Technological Exit: The Coming Battles Over Decommissioning
The new mandate includes identifying and decommissioning “obsolete” technologies.
This is scientifically complex and politically volatile.
Evidence of obsolescence is rarely binary, and removing entrenched interventions requires behavioural change, workforce retraining, and pathway redesign—areas where NICE has limited implementation leverage.
International Comparison: The UK Falling Behind Innovation Leaders
Other European systems have already adapted to the realities of modern technology cycles:
- Germany (DiGA, NUB, innovation fund): conditional reimbursement with structured RWE follow-up.
- France (PECAN, RIHN): temporary access pathways with mandated data collection.
- Netherlands (ZIN CED): early access tied to rigorous but feasible RWE frameworks.
These models acknowledge that waiting for mature evidence before reimbursement suppresses innovation.
England’s reliance on pre-adoption appraisal—without an equivalent conditional reimbursement mechanism—creates systemic drag.
The Central Paradox
If NICE is expected to simultaneously:
- appraise exponentially more technologies,
- govern digital and AI safety,
- set value-based tariffs,
- decommission outdated care, and
- maintain methodological gold standards…
…then without a radical expansion of analytical capacity, digital infrastructure, and workforce expertise, the organisation becomes the bottleneck rather than the accelerator.
The risk is not theoretical. It is structurally modelled in every OECD system where HTA responsibilities expanded without proportionate investment.
NICE is being asked to deliver 2035 innovation with 2015 capacity.
Unless this gap is closed, the very reforms designed to accelerate technology adoption may instead institutionalise delay.
The Productivity Obsession: Insourcing as the New NHS Capacity Engine
With 7.7 million patients on elective waiting lists, the NHS faces a structural capacity deficit that cannot be solved by traditional scheduling or marginal efficiency gains. Within this context, insourcing—the deployment of additional clinical teams to run existing NHS theatres during evenings, weekends, and bank holidays—has evolved from a temporary workaround into a core component of the elective recovery strategy.
Unlike outsourcing to private hospitals (Spire, Ramsay, Circle), insourcing retains NHS infrastructure, governance, safety protocols, and data flows, allowing trusts to expand throughput without fragmenting care pathways or losing clinical accountability.
Clinical: A Case Study in High-Performance NHS Insourcing
1Clinical represents the most mature form of insourcing in the UK, delivering full consultant-led surgical teams capable of running entire operating lists on:
- Weekends
- Evenings
- Bank holidays
- High-Volume/Low-Complexity (HVLC) hubs
Because activity remains inside NHS estates, this model preserves:
- NHS infection control standards
- NHS anaesthetic protocols
- NHS perioperative governance
- Full data capture for GIRFT benchmarking
This is fundamentally different from outsourcing, where cost, coding, case mix, and outcomes often diverge across providers.
What Insourcing Actually Enables (Backed by Capacity Science)
Insourcing allows trusts to unlock the latent elasticity of their own estates—moving theatres closer to the productivity envelope modelled in GIRFT and HVLC programmes.
1. Theatre Utilisation of 80–90%
NHS theatres often operate at 55–65% utilisation on weekdays because of staffing patterns, late starts, list overruns, and emergency pressures.
Insourcing provides pre-assembled, specialist teams who start on time, finish on time, and deliver predictable volume.
2. Reduction in Elective Backlogs
HVLC-compatible specialties—orthopaedics, ophthalmology, general surgery, ENT, urology—can gain substantial volume uplift through concentrated weekend operating lists.
3. Continuity of Governance and Safety
Because care occurs on NHS premises under NHS protocols, trusts retain control over:
- surgical site infection metrics
- consent and documentation
- safeguarding and incident reporting
- perioperative and anaesthetic governance
4. Preventing Capacity Collapse
Insourcing stabilises throughput in hospitals struggling with:
- consultant vacancies
- junior doctor rota gaps
- peak winter cancellations
- estate limitations that prevent new theatre builds
5. Alignment With GIRFT & Elective Recovery Frameworks
Insourcing is directly compatible with:
- HVLC pathways (ophthalmology, MSK, general surgery)
- theatre productivity dashboards
- elective recovery targets and 18-week RTT trajectories
It is one of the few interventions with immediate impact on backlog dynamics.
Other Key UK Insourcing Providers
- Medefer — virtual outpatient triage, digital referral optimisation
- Practice Plus Group — surgical hubs, accelerated elective pathways
- Totally Healthcare — dermatology, diagnostics, elective recovery
- NewMedica — ophthalmology surgical hubs and HVLC innovation
- SurgEase Innovations — mobile and modular operating theatres
These organisations collectively form the emerging NHS capacity ecosystem.
Why Productivity Alone Cannot Save the NHS
Insourcing improves flow, but cannot correct the structural capacity deficit.
The NHS faces limitations that productivity programmes cannot resolve:
1. Workforce Burnout & Attrition
You cannot expand surgical volume indefinitely with a shrinking workforce.
NHS England’s own projections show continued deficits in:
- theatre nurses
- anaesthetists
- consultant surgeons
- recovery staff
Insourcing mobilises external teams, but the core workforce remains overstretched.
2. Estate Decay and Infrastructure Deficit
Many hospitals operate with:
- undersized recovery units
- failing ventilation systems
- ageing theatres not HVLC-compatible
- insufficient pre-op assessment capacity
Productivity cannot compensate for physical constraints.
3. Insufficient High-Acuity Capacity
Elective surgery depends on the availability of:
- ICU beds
- enhanced recovery beds
- step-down capacity
The UK has one of the lowest ICU bed ratios in Western Europe.
You cannot improve surgical throughput if postoperative escalation bed availability remains static.
4. Productivity Without Resilience
Insourcing boosts volume, but it does not build resilience.
It is a treatment for symptoms, not the structural pathology.
The Core Insight
Insourcing is now a vital survival mechanism for NHS elective recovery.
But it is not—and cannot be—a substitute for:
- workforce expansion,
- estate renewal,
- critical care capacity,
- or long-term capital investment.
Productivity buys time.
It does not buy sustainability.
Year-of-Care Payments: Elegant in Theory, Fragile in Practice
Year-of-care (YoC) bundled payments—central to the 10-Year Plan—are presented as a modern, innovation-friendly reimbursement model designed to incentivise integration, prevention, continuity, and digital-first care. They promise a shift away from activity-based tariffs toward outcomes-based financing aligned with AI-driven triage, remote monitoring, and population health management.
But the scientific reality is more complex: chronic illness is non-linear, multimorbid, and behaviourally variable, making fixed annual tariffs extremely difficult to price with accuracy or fairness. The underlying assumption—that long-term conditions follow predictable cost curves—is contradicted by decades of epidemiological evidence.
Assigning a single annual tariff for patients with:
- COPD
- Heart failure
- Type 1 or Type 2 diabetes
- Frailty syndromes
- Multimorbidity clusters
…is analogous to pricing stochastic volatility as if it were a stable process. Chronic disease trajectories contain abrupt inflection points—exacerbations, hospital admissions, comorbidity emergence, polypharmacy effects—that do not conform to smooth actuarial models.
Why Bundled Payments Introduce Systemic Risk
1. Selective Enrolment — The Quiet Threat to Equity
Providers under YoC tariffs may preferentially enrol patients with low predicted variability.
Complex, unstable, or socioeconomically disadvantaged patients become financially “toxic” under fixed reimbursement.
This is a known behavioural response in international capitated systems.
2. Risk Aversion to Innovation in Complex Populations
Innovation—AI-enabled remote monitoring, digital disease-management tools, genomic risk stratification—depends on high-risk, high-need cohorts.
But YoC tariffs incentivise providers to avoid these exact groups, suppressing the diffusion of new technologies where they are most needed.
3. Algorithmic Rationing and Digital Gatekeeping
Bundled payments can drive subtle forms of rationing through:
- risk-score thresholds,
- algorithmic triage,
- digital decision rules,
- remote monitoring minima.
Digital pathways meant to expand access risk becoming tools of exclusion, particularly when ICSs operate under severe budget constraints.
4. Under-Treatment Incentives: The Dark Side of “Efficiency”
Because YoC payments reward spending less than the fixed budget, under-delivery of care can appear financially efficient.
Patients with fluctuating disease may receive fewer interventions, reduced community support, or limited diagnostics when budgets tighten.
5. ICSs Becoming Quasi-Insurers
Integrated Care Systems (ICSs), evolving into Integrated Health Organisations (IHOs), assume financial risk under YoC models.
Over time, their behaviour may resemble insurance entities rather than universal public care providers:
- premium-like risk segmentation
- actuarial forecasting
- exclusion of high-cost cases
- reliance on digital surveillance to control utilisation
This represents a drift toward insurance logic inside a universal system, without the explicit regulatory safeguards that social insurance countries (France, Netherlands, Germany) employ.
Why Innovation Is Particularly Vulnerable Under Year-of-Care Models
Innovation—especially in AI, diagnostics, genomics, and digital therapeutics—is disproportionately used in:
- high-risk patients
- unstable multimorbid populations
- those requiring continuous monitoring
- complex care pathways
YoC tariffs may unintentionally suppress adoption because:
- Innovative tools add short-term cost (even if long-term savings are significant).
- ICSs operating under fixed budgets become risk-averse to new technologies.
- RWE generation becomes fragmented when high-risk patients are excluded.
- Digital-first pathways are redesigned to control costs, not necessarily to improve outcomes.
Innovation thrives when the system rewards early adoption with real-world evaluation.
Year-of-care bundles reward predictability and cost containment.
The Structural Danger
In a universal NHS, reimbursement redesign must strengthen equity.
But YoC bundles risk creating:
- postcode-dependent access,
- risk-based triage,
- reduced uptake of novel technologies,
- and a quiet erosion of universality.
Without safeguards—conditional reimbursement (CED), risk adjustment for multimorbidity, innovation uplifts, and mandated RWE collection—the NHS could unintentionally shift toward a quasi-insurance model, where innovation becomes optional and high-risk patients quietly fall through the cracks.
Regional Health Innovation Zones: Reform or Repetition?

Innovation Zones are intended to be “living laboratories” for:
- AI-enabled pathways
- New reimbursement models
- Population health analytics
- Bundled payments
- Digital-first care pathways
But the NHS has seen this before:
- Vanguards
- STPs
- Integrated Care Pilots
Evaluations repeatedly found:
- Short political half-lives
- Poor scaling
- Weak data infrastructure
- Fragmented leadership
What These Zones Need to Succeed
- Long-term political insulation
- Freedom to fail & iterate
- Central evaluation architecture
- Real-world evidence frameworks (CED)
Otherwise, innovation zones become risk-transfer zones, shifting financial experimentation onto overstretched local systems.
The Missing Foundations: Workforce, Infrastructure, Reality
Digital transformation dominates the 10-Year Plan—but the foundations are decaying.
Workforce
- 120,000+ vacancies
- Junior doctor & consultant strikes
- Burnout and early retirement
- International competition for talent
Infrastructure
- No funded estate strategy
- Ageing hospitals
- Insufficient ICU capacity
- Shortage of diagnostic equipment
The Unspoken Question
Is the NHS financially sustainable on current terms?
Most European systems maintain universalism with modest co-payments or insurance contributions.
Examples:
- France – 70–80% base reimbursement + mutuelle
- Netherlands – compulsory social insurance
- Germany – solidarity GKV insurance
These models protect equity while ensuring capital elasticity and workforce reinvestment.
A System Drifting from Universalism to Modularity
Digital-first pathways, regional tariffs, and productivity-linked funding produce a technically universal, functionally unequal NHS.
Postcode, digital literacy, and local commissioning now influence access more than entitlement.
Universalism is being gradually replaced by regional modularity.
2035: A Choice, Not a Destiny
The NHS of 2035 will combine:
- AI diagnostics
- Precision genomics
- Predictive analytics
- Virtual care
But the real question is:
Can technology transform without dehumanising?
The Three Choices
- Efficiency vs. Empathy
- Innovation vs. Inclusion
- Data vs. Dignity
The NHS must choose whether innovation will serve people or merely processes.
healthcare reform must balance scientific evidence with human experience.
Innovation and the NHS: The Coming Capacity and Equity Divide
The debate about innovation and the NHS is no longer theoretical; it is a live test of whether a universal health system can absorb rapid advances in AI, genomics, digital diagnostics and new reimbursement models without losing its founding principles. The 10-Year Plan positions NHS innovation as the engine of future care, promising precision pathways, smarter diagnostics and more productive elective services. Yet innovation in the NHS cannot succeed on ambition alone. It requires analytical capacity, clinical workforce stability, digital infrastructure, and payment models that reward improvement rather than risk avoidance.
NICE’s expanding mandate illustrates this tension clearly. What was once a selective evidence gatekeeper now risks becoming an innovation bottleneck—not because the institution is failing, but because the volume and complexity of modern technologies outstrip the system built to evaluate them. In parallel, insourcing has become the emergency mechanism that keeps surgical services moving, demonstrating that NHS innovation often emerges pragmatically, not programmatically. But insourcing, no matter how effective, cannot compensate for structural shortages in workforce, estates or critical-care capacity.
Year-of-care tariffs add another layer of complexity. These bundled payments are designed to align innovation and the NHS by rewarding integrated, preventive care. Yet chronic illness does not behave predictably. Without safeguards, bundled payments risk suppressing the very digital innovations—remote monitoring, AI triage, personalised care pathways—that are essential to modern NHS reform. Instead of accelerating progress, poorly calibrated tariffs may push ICSs into insurer-like behaviour, quietly rationing care and narrowing access for high-need patients.
This is the central paradox of NHS innovation: the system is being asked to modernise faster than its foundations can support. The lesson, therefore, is not to limit innovation but to build the conditions that allow it to flourish. That means expanding NICE’s analytical capability, adopting conditional reimbursement pathways, investing in estates and the workforce, embedding real-world evidence frameworks, and ensuring digital tools strengthen inclusion rather than segmentation.
If policymakers can align innovation and the NHS with structural investment, governance reform and realistic capacity planning, the system can emerge stronger, more agile and more humane. If not, innovation will continue—but the NHS may struggle to hold together around it. The next decade will reveal whether innovation reshapes the NHS, or whether the NHS learns to reshape innovation on its own terms.
References & Further Reading
- UK Government / NHS England – Fit for the Future: 10-Year Health Plan for England (2025)
The official policy narrative behind the new 10-year direction for the English NHS, outlining “three fundamental shifts” in prevention, productivity and digital transformation, and setting out over 200 commitments for reform. Useful for anchoring any critique of year-of-care payments, productivity targets and digital-first pathways in the Government’s own language.
https://www.longtermplan.nhs.uk/ NHS Long Term Plan+1 - NHS England – The NHS Long Term Plan (2019)
The predecessor to the new 10-Year Plan; still the core reference for integrated care systems (ICS), prevention, and digitally enabled care. Comparing the 2019 Long Term Plan with the 2025 Ten-Year Plan helps show how much is genuinely new versus rebranded continuity.
https://www.longtermplan.nhs.uk/ NHS Long Term Plan+1 - NHS England – Reforming Elective Care for Patients (2025)
Sets out proposals to restore the 18-week RTT standard and explains how surgical hubs, insourcing, high-volume low-complexity (HVLC) lists and GIRFT will be used to recover elective backlogs. This is a key policy hook for your section on weekend surgery, insourcing providers and “productivity as salvation”. https://www.england.nhs.uk/long-read/reforming-elective-care-for-patients/ NHS England+1 - Getting It Right First Time (GIRFT) – National Improvement Programme
GIRFT is the national NHS programme that uses benchmarking, pathway redesign and theatre utilisation data to drive efficiency and quality in surgical care. It directly underpins the elective recovery and insourcing narrative, making it a useful evidence base for claims about high-volume weekend operating and theatre optimisation.
https://gettingitrightfirsttime.co.uk/ Getting It Right First Time – GIRFT+1 - NICE – “Should NICE’s cost-effectiveness thresholds change?” (2024 blog)
A key piece in the contemporary debate over whether NICE’s long-standing £20–30k/QALY threshold remains appropriate. The blog explains NICE’s rationale for a threshold range and acknowledges growing pressure to adjust it, which dovetails with your arguments about innovation bottlenecks and undervaluation of new therapies and diagnostics.
https://www.nice.org.uk/news/blogs/should-nice-s-cost-effectiveness-thresholds-change- NICE+1 - NICE – Changes to cost-effectiveness thresholds (news, 2025)
Confirms that NICE plans to move to a £25,000–£35,000/QALY range once the legal framework permits, marking one of the most significant methodological shifts in two decades. This is highly relevant for your FAQ section on NICE thresholds and for contrasting the UK with more flexible European HTA models.
https://www.nice.org.uk/news/articles/changes-to-nice-s-cost-effectiveness-thresholds-confirmed NICE - NHS England – Digital Technology & Transformation Resources
The main portal for NHS England’s digital transformation work, including EHR interoperability, AI triage, virtual wards and population health tools. It’s the right “real-world” link for claims about digital-first pathways, remote monitoring and data-driven decision-making in your 10-Year Plan discussion.
https://www.england.nhs.uk/digitaltechnology/ NHS England - NHS England – Children & Young People Elective Recovery Toolkit
An example of how elective recovery is being operationalised through dashboards, data-driven prioritisation and pathway redesign. This supports your argument that dashboards and productivity tools can improve throughput but may still struggle against workforce and estate constraints.
https://www.england.nhs.uk/long-read/children-and-young-peoples-elective-recovery-toolkit/ NHS England+1 - NHS England – Long Term Conditions Year of Care Commissioning Programme Handbook
A foundational handbook on “year-of-care” commissioning models for chronic disease, explaining the logic, contract structure and data requirements. It’s an excellent technical reference for your critique of bundled payments and the difficulty of pricing multimorbidity and complexity.
https://www.england.nhs.uk/wp-content/uploads/2017/02/ltc-yoc-handbook.pdf NHS England - Nuffield Trust – The NHS Payment System: Evolving Policy and Emerging Evidence (2014)
Although slightly older, this report remains one of the clearest analyses of how payment structures (PbR, pathway payments, year-of-care) shape behaviour in the NHS. It explicitly discusses experimentation with bundled contracts and provides the conceptual backbone for your “elegant theory, complex reality” section.
https://www.nuffieldtrust.org.uk/research/the-nhs-payment-system-evolving-policy-and-emerging-evidence Nuffield Trust - Nuffield Trust – Ten Year Plan for the English NHS / Financial & Capacity Analysis
Commentaries and briefings from Nuffield Trust unpack the affordability, workforce and capacity implications of the 10-Year Plan, including concerns about funding shortfalls and productivity assumptions. These are ideal for backing up your warnings about “statistical efficiency at the expense of moral entropy”.
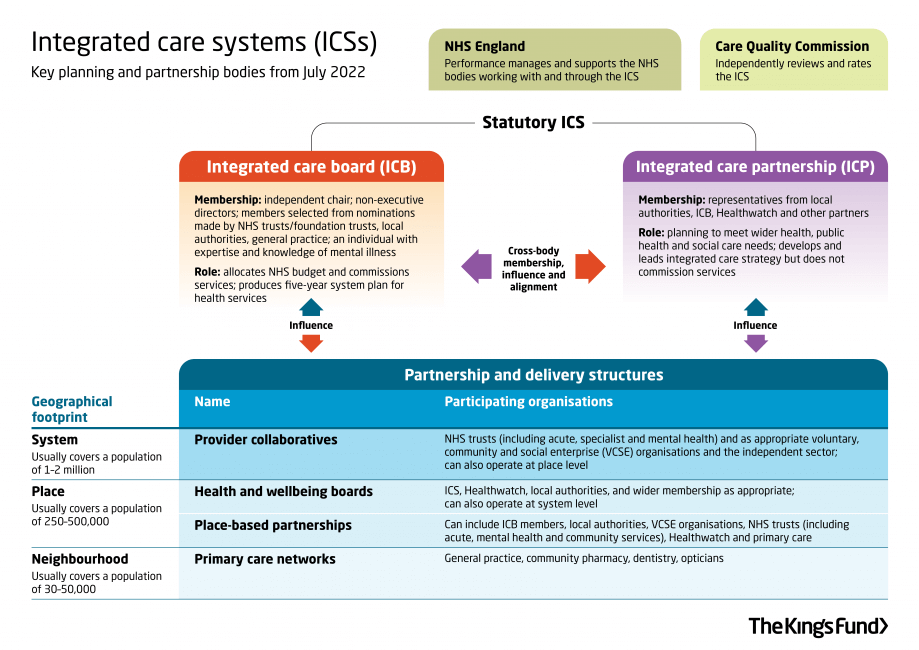
https://www.nuffieldtrust.org.uk/ LinkedIn+1 - The King’s Fund – Integrated Care Systems Explained (2022)
A definitive long read on what ICSs are, how they are supposed to function, and where the governance/accountability tensions lie. It directly supports your discussion of Integrated Health Organisations (IHOs), regional payment models and the drift toward modularity.
https://www.kingsfund.org.uk/insight-and-analysis/long-reads/integrated-care-systems-explained The King’s Fund+1 - The King’s Fund – Realising the Potential of Integrated Care Systems (2024)
Focuses on ICS workforce, collaboration and delivery challenges. Useful for linking your workforce crisis narrative with the structural realities of ICSs acting as de facto regional payers and planners.
https://www.kingsfund.org.uk/insight-and-analysis/reports/integrated-care-systems-workforce The King’s Fund - Health Foundation – “Can the NHS meet its 2% productivity challenge?” (2025 blog)
A timely analysis of whether the NHS can realistically deliver the productivity gains that underpin current funding and reform assumptions. This is a perfect reference for your “productivity obsession” section and for framing insourcing as necessary but insufficient.
https://www.health.org.uk/features-and-opinion/blogs/can-the-nhs-meet-its-2-productivity-challenge-here-s-what-experts-think Health Foundation+1 - Health Foundation – Falling Short: The NHS Workforce Challenge
Annual workforce trend reports that document the scale of shortages, recruitment gaps and retention problems across nursing, general practice and key specialties. These are your best evidence base for the argument that the “real crisis is human capital erosion, not digital lag”.
https://www.health.org.uk/reports-and-analysis/reports/falling-short-the-nhs-workforce-challenge Health Foundation+1 - Health Foundation – NHS Workforce Projections 2022–2030
Provides modelled projections of supply and demand for NHS staff to 2030/31, under different policy scenarios. It is especially useful for quantifying how far current plans fall short of what is needed to sustain a digitally transformed NHS.
https://www.health.org.uk/reports-and-analysis/reports/nhs-workforce-projections-2022 Health Foundation - OECD Health Statistics – Hospital Beds, ICU Capacity & Spending
The primary comparative dataset for hospital and ICU beds per 1,000 population, health expenditure as a share of GDP, and capital investment. Use this to substantiate your cross-country comparisons with France, Germany and the Nordics. https://stats.oecd.org/ - Office for National Statistics (ONS) – UK Health & Care Expenditure
The official source for UK health expenditure, public spending trends and long-run demographic pressures. This underpins your claims about funding levels relative to GDP and international peers.
https://www.ons.gov.uk/ - NHS England – Board & Leadership Team
Provides the governance context for accountability, decision-making and strategic direction under the 10-Year Plan, including the evolving relationship between NHS England, DHSC and ICSs.
https://www.england.nhs.uk/about/nhs-england-board/our-leadership-team/ NHS England+1 - Health Foundation – Labour’s First Year: Health Policy & Payment Reform (2025)
Explores early moves toward new payment models, including proposals for year-of-care payments and whole-population budgets for certain providers. This neatly reinforces your concern that IHOs could become quasi-insurers without explicit safeguards.
https://www.health.org.uk/ Health Foundation+1 - NHS England – GIRFT & High Volume Low Complexity (HVLC) Programme
Detailed resources on how GIRFT and HVLC pathways are being used to restructure elective surgery, concentrate activity in hubs and support weekend and evening lists. This is an excellent “real-world” link for your insourcing and weekend surgery narrative.
https://gettingitrightfirsttime.co.uk/hvlc/hvlc-programme/ Getting It Right First Time – GIRFT+1 - Odelle Technology – NHS Reform, Evidence & Reimbursement Insights
Odelle’s own analysis of NHS coding, tariffs, HRGs, AI diagnostics and market access. Internally linking to this content strengthens your SEO for “NHS reimbursement”, “HRG tariffs”, “NICE and HTA”, and positions Odelle as a thought leader on the intersection of evidence, economics and reform.
https://www.odelletechnology.com/
FAQ — The NHS 10-Year Plan Paradox (2025–2035): Reimbursement, Innovation, and the Coming Bottleneck
Q1. What is the NHS 10-Year Plan and why is it creating a paradox for innovation?
The NHS 10-Year Plan (2025–2035) aims to create a digitally enabled, outcomes-driven, productivity-centred health system.
The paradox is simple:
While the Plan promises innovation, AI adoption and streamlined care, it introduces new layers of regulation, reimbursement redesign and NICE oversight that may slow adoption rather than accelerate it.
Ambition is high, but the implementation risks creating an innovation bottleneck—especially in diagnostics, digital health, and AI tools.
Q2. Why is NICE becoming both a bridge and a bottleneck in the future NHS?
Under the 10-Year Plan, NICE must:
- Evaluate every diagnostic, device and digital technology
- Manage technology decommissioning
- Oversee value-based reimbursement
- Expand its appraisal pipeline at industrial scale
But NICE was never designed as a high-volume factory.
Without major investment in capacity, data systems and reviewers, the expanded mandate risks turning NICE into the key chokepoint in NHS innovation, delaying access to AI diagnostics, genomics, and digital tools.
Q3. What are Year-of-Care (bundled) payments and why are they controversial?
Year-of-Care payments give providers one annual tariff per patient for conditions like COPD, heart failure, diabetes or multimorbidity.
While elegant in theory, bundled tariffs risk:
- Risk selection (avoiding complex patients)
- Under-provision to preserve budget surpluses
- Algorithmic rationing
- Insurance-style behaviour in ICSs
Real-world NHS pathways remain fragmented, making fixed annual reimbursement financially unstable and clinically risky.
Q4. How does the 10-Year Plan affect NHS reimbursement structures?
The Plan shifts reimbursement towards:
- Outcomes-based tariffs
- Productivity-linked funding
- Year-of-care bundles
- Digital pathway incentives
- Regional flexibility within ICSs
This marks a move from simple activity-based tariffs to complex reimbursement ecosystems, where payment depends on performance, outcomes, and digital integration.
Q5. What role do Integrated Care Systems (ICSs) play in this new landscape?
ICSs are evolving into Integrated Health Organisations (IHOs)—regional bodies that act as quasi-payers.
Under the 10-Year Plan, ICSs increasingly control:
- Local budgets
- Contracting models
- Risk-sharing frameworks
- Adoption of digital tools and diagnostics
This shift risks creating postcode-dependent access, challenging the NHS principle of national equity.
Q6. Why is NHS productivity at the centre of the 10-Year Plan?
The Government expects the NHS to deliver a 2% productivity increase annually.
This has driven the rise of:
- Weekend surgery
- Insourcing providers (1Clinical, Practice Plus Group, NewMedica)
- Modular theatres
- AI-enabled scheduling
- Elective surgical hubs
However, productivity gains alone cannot overcome workforce shortages, estate decay and ICU capacity limits.
Q7. Why might innovation—especially digital health and AI—actually slow down?
Because innovation now requires:
- NICE approval
- Digital technology assessment
- Data interoperability compliance
- Cybersecurity validation
- Workforce readiness
- Economic modelling for reimbursement
Each step adds time and complexity.
Innovation risks becoming bureaucratised, not accelerated.
Q8. Why does the UK underperform in cancer, ICU capacity, and diagnostic speed?
Compared to France, Germany and the Nordics, the UK has:
- Fewer hospital beds
- Lower ICU capacity
- Older diagnostic equipment
- Severe workforce shortages
- Slower technology adoption through NICE
The NHS delivers equity, but at the cost of capacity and speed.
Q9. What are Regional Health Innovation Zones, and will they work?
These zones are designed to pilot:
- New payment models
- AI-enabled pathways
- Digital-first care
- Population analytics
However, previous NHS pilot programmes (Vanguards, STPs, Integrated Care Pilots) suffered:
- Short evaluation cycles
- Rapid political turnover
- Poor data architecture
Unless Innovation Zones receive long-term protection and robust evaluation structures, they risk becoming risk-transfer zones, not reform engines.
Q10. How might NHS funding need to change to remain sustainable?
The politically sensitive reality is that the UK may require a shift toward European-style mixed funding, including:
- Modest co-payments
- Personalised prevention subscriptions
- Optional digital service tiers
- Expanded social insurance contributions
France, Sweden, Germany and the Netherlands maintain high equity with co-financing, unlike the UK’s single-tax model.
Q11. Why does digital transformation risk worsening health inequalities?
Digital-first pathways assume:
- Smartphone access
- Digital literacy
- Stable Wi-Fi
- Familiarity with portals and apps
This can marginalise:
- Older adults
- Rural populations
- Lower-income groups
- Digitally excluded communities
Transformation without inclusion becomes digital exclusion.
Q12. What is driving the NHS workforce crisis?
Key pressures include:
- 120,000+ vacancies
- Pay erosion
- Burnout
- International competition
- Lack of retention strategies
- Limited career development
The 10-Year Plan emphasises digital innovation, but no digital tool replaces human capital.
Q13. Why do NHS innovation pilots fail to scale?
Because the NHS prototypes innovation in short political cycles, not long-term evaluation frameworks.
Unlike Germany’s DiGA and France’s PECAN registries, the NHS lacks:
- Standardised data capture
- Longitudinal outcomes tracking
- Consistent funding streams for evaluation
As a result, pilots become islands of excellence without bridges.
Q14. Will the NHS introduce patient payments or insurance-style mechanisms?
This remains taboo politically, but experts increasingly argue that small, structured contributions—as used across Europe—could stabilise NHS finances.
Without reform, waiting lists and workforce attrition may produce de facto privatisation via delays, even if the NHS remains “free”.
Q15. What must the NHS do to avoid an innovation bottleneck by 2035?
To remain both equitable and innovative, the NHS must:
- Expand NICE capacity
- Adopt conditional reimbursement (CED)
- Prioritise digital inclusion
- Increase capital investment
- Rebuild the workforce
- Introduce sustainable funding mechanisms
Innovation requires infrastructure, not slogans—and reform must balance creativity in reimbursement with compassion in care.