
Medical purpose, MiGeL and price discipline
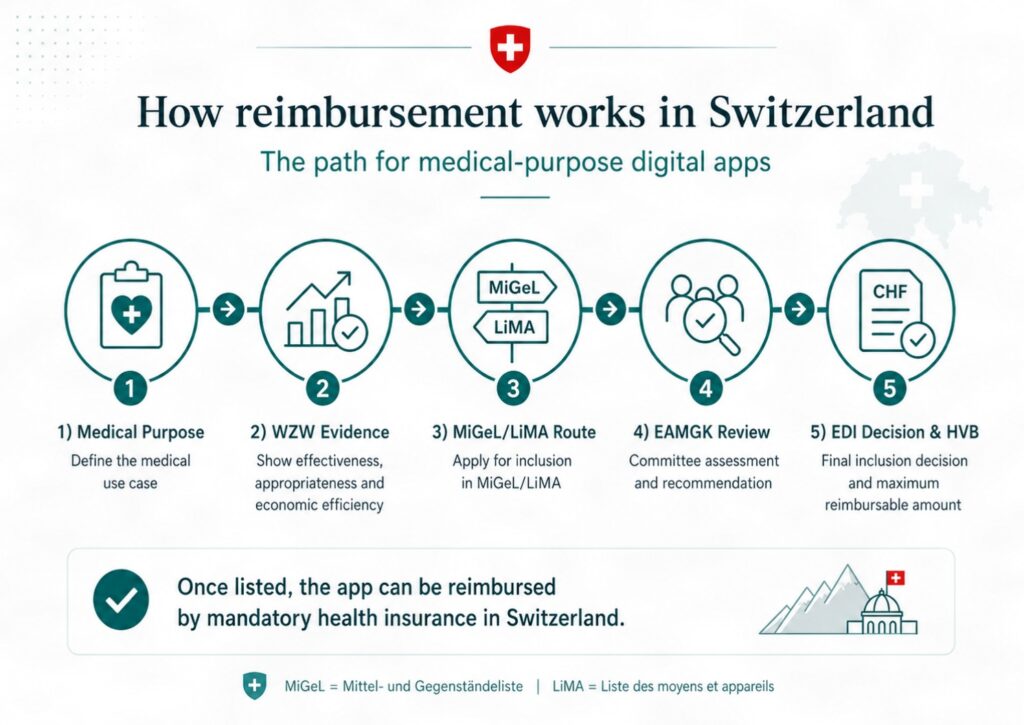
From 1 July 2026, Switzerland will introduce reimbursement for selected medical-purpose digital health applications through MiGeL/LiMA. This article explains how companies should approach Swiss digital app reimbursement, including OKP eligibility, WZW evidence, MiGeL submission and HVB price calculation.
From 1 July 2026, Switzerland will do something quietly important in digital health reimbursement.
It will not become Germany.
It will not create a broad DiGA-style directory.
It will not reimburse wellness apps, lifestyle tools, meditation products or digital coaching platforms simply because they live on a phone.
Instead, Switzerland is doing something more precise, more cautious and arguably more payer-disciplined.
It is creating a formal route for selected medical-purpose digital health applications to be reimbursed through the existing Swiss compulsory health insurance system, using the MiGeL/LiMA framework — the list of reimbursed means and devices.
The first visible opening is narrow: interactive digital cognitive behavioural therapy applications for adults with mild-to-moderate depression or recurrent depressive disorder, used either alongside psychotherapy or as a bridge while patients are waiting for psychotherapy.
That narrowness is not a weakness.
It is the signal.
Switzerland is not saying that apps should be reimbursed because they are digital. It is saying that a digital application may be reimbursed when it has a medical purpose, fits a recognised clinical pathway, satisfies the Swiss requirements of effectiveness, appropriateness and economic efficiency, and can be priced with real price discipline.
For digital health companies, the question changes.
The question is no longer: “Can my app be reimbursed in Switzerland?”
The better question is:
Can my app behave like a reimbursable medical intervention?
The first test: medical purpose
Switzerland begins with classification.
Some digital tools are general wellness products. They support fitness, sleep, relaxation, nutrition, mindfulness or lifestyle behaviour. They may be useful. They may even be commercially successful. But they are not usually a matter for compulsory health insurance.
Other apps support patients with education, information, disease understanding or self-management. These may enter the reimbursement discussion if their function moves beyond generic support and begins to perform a medical role.
The decisive category is the digital health application with a medical purpose.
This includes software, apps, connected devices, sensor-based systems, AI-enabled tools or combinations of these used for prevention, diagnosis, monitoring, prognosis, treatment, alleviation or care of disease.
That phrase — medical purpose — is the first gate.
A company should not begin a Swiss reimbursement strategy with screenshots, downloads or user engagement.
It should begin with the medical claim.
What disease is being addressed?
Which patient population is eligible?
What clinical function does the app perform?
What decision, behaviour, symptom, treatment or pathway step does it change?
Why is this a healthcare intervention rather than a digital convenience?
If the medical purpose is vague, the reimbursement case will be weak.
The second test: where the app belongs in the Swiss system

Switzerland is not building a separate digital-app universe.
It is fitting digital applications into the existing structure of compulsory health insurance.
That is why the route depends on how the app is used.
If the app is simply part of a physician’s service, it may sit inside physician-service logic.
If it is part of a non-physician healthcare service, the question becomes whether that provider and service are recognised under the Swiss system.
But if the app is used directly by the patient, as many digital therapeutics are, the key route is MiGeL/LiMA.
MiGeL is Switzerland’s list of means and devices reimbursed by compulsory health insurance. It has traditionally dealt with physical medical products used at home or in care settings. Switzerland is now adapting that structure to selected digital health applications with a medical purpose.
This is the true Swiss innovation.
Not a consumer app list.
Not a digital sandbox.
Not a broad early-access scheme.
A patient-used medical app may be treated as a reimbursable medical product, with a defined position and a maximum reimbursable amount.
For companies, the practical task is therefore to show that the application fits the MiGeL logic.
It must be patient-usable.
It must have a medical purpose.
It must support treatment, monitoring, self-management or another recognised medical function.
It must satisfy Swiss evidence and safety expectations.
It must be capable of being described in a category that makes sense for compulsory insurance.
This is not app-store thinking.
It is benefit-category thinking.
The third test: WZW
Swiss reimbursement turns on three letters:
WZW — Wirksamkeit, Zweckmässigkeit, Wirtschaftlichkeit.
Effectiveness.
Appropriateness.
Economic efficiency.
This is where many digital health companies will need to change their language.
Engagement is not enough.
Downloads are not enough.
Patient satisfaction is not enough.
A beautiful interface is not enough.
The application must show that it works, that it is suitable for the intended patient group and pathway, and that the proposed reimbursement is economically defensible.
For a therapeutic app, the evidence should address clinical effect, safety, appropriate patient selection, duration of use, supervision, discontinuation, risk management and practical integration into care.
For a monitoring app, the evidence burden is different but no less important. The key issue is actionability.
A monitoring app that collects symptoms or physiological data must have a credible response pathway.
What happens when the data are abnormal?
Who sees them?
Who acts?
What is the escalation plan?
What are the risks of false reassurance or unnecessary intervention?
Swiss guidance explicitly recognises the problem of false negatives and false positives in monitoring. A false negative can miss deterioration. A false positive can create anxiety, further tests and additional costs.
This is why a digital health application needs more than data capture.
It needs clinical logic.
The fourth test: pathway role
Every reimbursed digital application needs a job in the pathway.
The Swiss depression example is useful because the pathway role is clear.
The product is not framed as a general mental health app. It is not a wellness companion. It is not broad digital coaching.
It is an interactive digital CBT application for a defined population, used either alongside psychotherapy or while patients are waiting for psychotherapy.
That is a reimbursement-quality claim.
It links the technology to a recognisable health-system problem: access to therapy, waiting times, structured treatment support and continuity of care.
Other digital health companies should learn from this.
A diabetes app should not simply say it improves self-management. It should explain whether it supports insulin dosing, hypoglycaemia avoidance, HbA1c improvement, time-in-range, therapy adherence or clinician review.
A cardiac app should not simply say it monitors patients. It should explain whether it identifies deterioration, prevents avoidable admissions, supports medication titration or enables safer follow-up.
An oncology app should not simply say it records symptoms. It should explain whether it changes escalation, toxicity management, relapse detection, emergency attendance or continuity between hospital visits.
The app must have a pathway job.
Without that, it is only software.
The fifth test: the submission route
For a patient-used medical app, the likely Swiss route is an application for inclusion or amendment within MiGeL/LiMA.
In practical terms, the dossier needs to be prepared for BAG review and then assessment by the relevant MiGeL committee structure within the Eidgenössische Kommission für Analysen, Mittel und Gegenstände EAMGK.
The committee assesses whether the criteria of effectiveness, appropriateness and economic efficiency are met. It then makes a recommendation to the Federal Department of Home Affairs EDI, which makes the final decision on changes to MiGeL.
If information is missing, the dossier can be returned for further work.
This matters because companies often imagine reimbursement as a single application form. In reality, it is a structured argument.
A good Swiss dossier should answer:
What is the medical purpose?
What is the target population?
What is the intended use?
Who prescribes or initiates the app?
Is the app self-used by the patient?
Does it qualify as a medical device where required?
What clinical evidence supports effectiveness?
Why is it appropriate for this pathway?
What is the economic justification?
What maximum reimbursement amount is being sought?
What comparator or anchor price is relevant?
How will the product be maintained, updated and secured over its lifecycle?
The strongest submissions will not simply describe the app.
They will describe the clinical intervention the app enables.
The sixth test: price discipline
The most interesting part of the Swiss approach may be pricing.
Switzerland recognises that software is not a box of medical devices.
A physical product usually carries material, manufacturing, storage, logistics and distribution costs every time another unit is supplied.
Software is different.
A digital therapeutic may require substantial investment in development, regulatory work, clinical evidence, cybersecurity, maintenance, updates, multilingual deployment and market access. But once built, its marginal cost per additional user can be relatively low.
That creates a payer problem.
If the price is too low at launch, serious digital therapeutics may never enter the market. If the price stays too high after scale is reached, the health system may overpay for software whose early investment costs have already been recovered.
Switzerland’s answer is the Höchstvergütungsbetrag, or HVB the maximum reimbursable amount.
The HVB is not simply the manufacturer’s requested price. It is a ceiling.
For digital health applications in MiGeL, the Swiss model looks at two main forms of logic.
The first is cost-based: what did it reasonably cost to develop, regulate, operate, maintain, support and adapt the application?
The second is comparator-based: what is the relevant anchor price, either from comparable digital applications or from an analogue therapy already reimbursed in Switzerland?
In simple terms, Switzerland asks two questions:
What does this product reasonably cost?
And what is it reasonably comparable to?
The maximum reimbursement amount is then disciplined by those reference points.
This is price discipline.
The seventh test: early price versus mature price
Switzerland also recognises that the economics of a digital therapeutic change over time.
At the beginning, the company may need to recover development, certification and market-entry costs. Later, if the product scales, those costs may be considered amortised, leaving mainly operating, maintenance and support costs.
The Swiss model therefore distinguishes between an early phase and a later phase.
In the early phase, the HVB can reflect market-entry economics.
In the later phase, once a threshold is reached, the reimbursement amount can be recalculated to reflect routine use.
This is sophisticated.
It gives room for innovation without allowing software pricing to drift away from economic reality.
It also means that companies should arrive with credible assumptions about Swiss utilisation, expected uptake, maintenance costs, support costs, regulatory costs, language requirements and comparable alternatives.
A reimbursement price will need to be argued, not asserted.
The depression precedent
The first major Swiss digital health position is deliberately narrow.
It covers interactive digital CBT applications for depression, for independent self-use by patients. The official MiGeL amendment defines the intervention, its CBT content, its eligible indications, age requirements, prescribing limitations, and the licence period.
The position covers mild and moderate depressive episodes, and recurrent depressive disorder with a current mild or moderate episode.
It does not cover severe depression.
That exclusion is important. It shows that Switzerland is not only opening a door; it is drawing boundaries around it.
The commentary also notes that the assessed product was deprexis, but the position is generic. Other products that meet the WZW criteria and the limitations may be reimbursed under the same position.
This is a critical detail.
Switzerland is not merely listing one branded app. It is creating a reimbursable category.
That is why the move matters.
How a company should prepare
A digital health company considering Switzerland should prepare the reimbursement case in a disciplined sequence.
First, define the medical purpose.
Second, define the patient population.
Third, map the clinical pathway.
Fourth, identify who prescribes, initiates or supervises use.
Fifth, determine whether the application is part of a professional service or a self-used patient application suitable for MiGeL.
Sixth, build the WZW evidence case.
Seventh, prepare the economic case.
Eighth, justify the proposed price using both cost information and comparator logic.
Ninth, show how the application will be maintained, updated, secured and monitored over its lifecycle.
Tenth, be ready for evaluation using real-world utilisation and price data.
This is not a digital marketing exercise.
It is a reimbursement dossier.
Why this matters
Switzerland’s move is easy to underestimate because it is not noisy.
There is no grand app directory.
No sweeping claim that all digital health tools should be reimbursed.
No slogan for every start-up slide deck.
But that is exactly why it matters.
Switzerland is showing how a mature payer system can absorb digital therapeutics without losing control of evidence, indication, pathway position or price.
It is also showing where digital health reimbursement in Europe may be heading.
The future will not belong to apps that merely collect data, educate patients or look modern.
It will belong to digital medical interventions that can answer payer questions with precision.
What is the medical purpose?
Who is the patient?
What is the pathway role?
What is the evidence?
What is the comparator?
What is the justified price?
What happens after scale?
For companies, Switzerland offers a clear lesson.
Do not try to sell the app.
Build the reimbursement argument around the intervention.
Because in Switzerland, the app is not the story.
The reimbursable medical purpose is.
And the price must survive price discipline.
Official references
- Bundesamt für Gesundheit BAG — Digitale Therapie-Angebote können neu von Krankenversicherung übernommen werden, 4 December 2025
https://www.bag.admin.ch/de/newnsb/GcAWd8OPd1eHCPFR5H8t3 - Bundesamt für Gesundheit BAG — Mittel- und Gegenständeliste MiGeL official page
https://www.bag.admin.ch/de/mittel-und-gegenstaendeliste-migel - Bundesamt für Gesundheit BAG — Änderungen Anhang 2 KLV MiGeL vom 2. Dezember 2025 per 1. Juli 2026
https://www.bag.admin.ch/dam/de/sd-web/PqAmz18kA63r/%C3%84nderungen%20Anhang%202%20KLV%20MiGeL%20vom%202.%20Dezember%202025%20per%201.%20Juli%202026.pdf - Bundesamt für Gesundheit BAG — Kommentar zu den Änderungen des Anhangs 2 KLV vom 2. Dezember 2025 per 1. Januar 2026, 1. Juli 2026 und 1. Januar 2027
https://www.bag.admin.ch/dam/de/sd-web/O3h2u2RlvQ4v/Kommentar%20zu%20den%20%C3%84nderungen%20des%20Anh.%202%20KLV%20vom%202.%20Dezember%202025%20per%201.%20Jan.%202026%201.%20Juli%202026%20und%201.%20Jan.%202027.pdf - Bundesamt für Gesundheit BAG — Faktenblatt: Vergütung von digitalen Gesundheitsanwendungen im Rahmen der OKP, November 2024
https://www.bag.admin.ch/dam/de/sd-web/qAvnbNFDJ6lY/faktenbatt-verguetung-dig-anwendungen-vers112024.pdf - Bundesamt für Gesundheit BAG — Berechnungsmodell für die Festsetzung des Höchstvergütungsbetrags HVB von digitalen Gesundheitsanwendungen dGA in der MiGeL, March 2026
https://www.bag.admin.ch/dam/de/sd-web/VYxrS1sjQsO6/2026_Berechnungsmodell_HVB%20von%20dGA%20in%20der%20MiGeL.pdf - Bundesamt für Gesundheit BAG — Bemessungsgrundlage: Vergütung von dGA gemäss KVG, 2026
https://www.bag.admin.ch/dam/de/sd-web/Q0WV9efLpfrX/2026_Bemessungsgrundlage_Verg%C3%BCtung%20von%20dGA%20gem%C3%A4ss%20KVG.pdf - Bundesamt für Gesundheit BAG — Entwicklung Bemessungsgrundlage: HVB von dGA in der MiGeL, 2026
https://www.bag.admin.ch/dam/de/sd-web/Of-3nB6ZoRz2/2026_Entwicklung%20Bemessungsgrundlage_HVB%20von%20dGA%20in%20der%20MiGeL.pdf