
Product-market fit gets attention. Evidence-market fit gets reimbursement, procurement and scale.
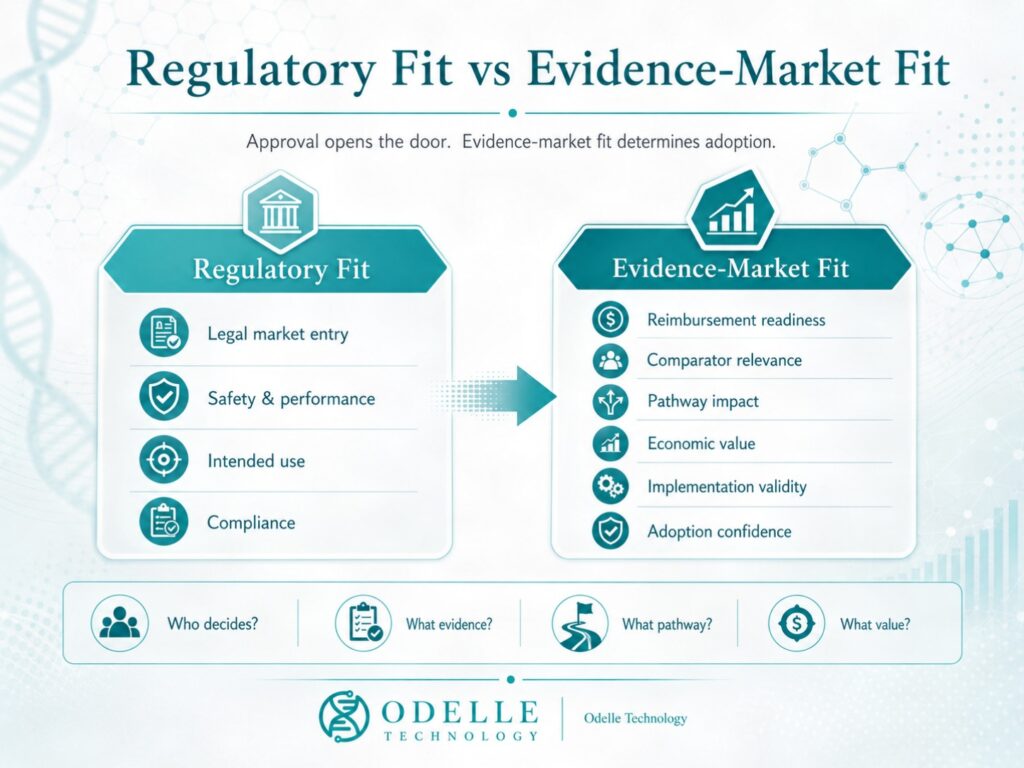
Regulatory approval may open the door. Evidence-market fit determines whether health systems will pay, procure, recommend or scale.
Many healthtech companies believe they have product-market fit.
Fewer can prove evidence-market fit.
That distinction is becoming one of the most important questions in health technology adoption.
Product-market fit means that users want the product. Clinicians may like it. Patients may engage with it. A hospital may pilot it. An investor may understand the commercial promise. Early customers may even pay.
But in healthcare, that is not enough.
Healthcare markets do not behave like ordinary consumer markets. A technology may be attractive, clinically interesting and commercially promising, yet still fail to achieve reimbursement, procurement, commissioning or scaled adoption if the evidence package does not match the expectations of the decision-maker.
Odelle definition

At Odelle Technology, we define evidence-market fit as the point at which a health technology’s evidence package matches the expectations of the decision-maker who must approve, reimburse, procure, recommend, commission or scale it.
That is a higher standard than product-market fit.
And it is becoming the new access discipline.
Key takeaways
- Product-market fit gets attention; evidence-market fit gets adoption.
- Regulatory clearance is not the same as reimbursement, procurement or commissioning readiness.
- The problem is often not missing evidence, but misaligned evidence.
- AI, digital health and medtech companies must prove pathway impact, implementation validity and economic value.
- Health systems are moving from innovation enthusiasm to evidence discipline.
- The companies that prepare evidence early will be better positioned for HTA, reimbursement, procurement and scale.
Why evidence-market fit matters now
Across the UK and Europe, health systems are moving away from innovation enthusiasm and towards evidence discipline.
The new MHRA–NICE aligned pathway is one clear signal. From 1 April 2026, the pathway became fully open for business. NICE describes it as a way of bringing licensing and value assessment closer together, so that medicines can reach NHS patients 3 to 6 months sooner. GOV.UK similarly explains that the pathway brings NICE decisions forward to align with the Medicines and Healthcare products Regulatory Agency, so that regulatory and health technology assessment decisions can be delivered at the same time.
This is not simply a faster process.
It is a convergence signal.
Regulatory approval and reimbursement assessment are moving closer together. Companies can no longer assume that market access begins after approval. The clinical evidence, payer story, economic model and access pathway need to be shaped much earlier.
The same shift is visible in digital health.
NICE’s Evidence Standards Framework for Digital Health Technologies is designed to provide evidence standards for a wide range of digital health technologies. NICE says evaluators and decision-makers can use the framework to identify technologies likely to offer benefits to users and to the health and care system.
This matters because digital health companies often have usability data, engagement data or pilot enthusiasm, but not always the evidence needed for commissioning, procurement or reimbursement.
The direction is even clearer in adult social care.
In May 2026, the UK Government announced that NICE had been commissioned to develop a new Evidence Standards Framework for Digital Care Technologies in adult social care. The Government identified a familiar problem: outcomes are measured inconsistently, much existing evidence comes from suppliers rather than independent evaluators, and there is no shared approach for assessing quality, impact or value. The new framework is intended to bring greater consistency and confidence to how evidence for care technologies is generated, assessed and used.
That is exactly the evidence-market fit problem.
A technology may be useful. It may have a compelling demonstration. It may even have enthusiastic users. But if the evidence is inconsistent, supplier-led, difficult to compare or poorly connected to real-world decision-making, adoption will remain fragile.
France is moving in a parallel direction.
HAS has developed a cadre de confiance — a trust framework — for digital technologies and AI systems used in care, including professional-use digital medical devices. HAS frames the work around supporting selection, proper use and evaluation so that useful and performant technologies can be integrated into the healthcare system.
The HAS and CNIL partnership signed in March 2026 strengthens this direction further, with a focus on good practices, personal data protection and fundamental rights linked to digital tools in health, social care and medico-social care.
Different countries. Different mechanisms. Same policy signal.
Health systems are no longer asking only whether a technology is innovative.
They are asking whether it is evaluable, adoptable, affordable, implementable and trustworthy.
That is evidence-market fit.
Regulatory fit is not evidence-market fit

One of the most common mistakes in health technology strategy is confusing regulatory fit with evidence-market fit.
Regulatory fit asks:
Can the product legally enter the market?
Evidence-market fit asks:
Can the product be trusted, funded, procured, recommended and scaled in the market?
These are not the same question.
A company may receive regulatory clearance and still lack a compelling reimbursement story.
A diagnostic may demonstrate analytical performance and still fail to prove clinical utility.
A digital therapeutic may show engagement and still lack evidence of durable outcome change.
An AI tool may show strong accuracy and still fail to demonstrate safe actionability in clinical workflow.
A medtech device may receive approval and still fail to show hospital budget impact or pathway value.
A social care technology may help in one pilot and still lack evidence that it can be implemented consistently across fragmented real-world care settings.
That is why evidence-market fit matters.
It sits between approval and adoption.
It is the bridge between technical promise and system confidence.
The problem is often not evidence absence. It is evidence misalignment.
Many companies do not lack evidence.
They have the wrong evidence.
A study measures engagement, but the payer needs avoided utilisation.
A pilot shows satisfaction, but the commissioner needs budget impact.
A diagnostic shows accuracy, but NICE needs clinical utility.
A hospital trial shows enthusiasm, but procurement needs affordability.
A digital tool shows usability, but the care provider needs implementation feasibility.
An AI system shows AUC, sensitivity or specificity, but the health system needs evidence of bias management, drift monitoring, workflow integration, escalation logic, patient safety and professional accountability.
This is the central problem.
Evidence is only valuable if it fits the decision.
A company does not have evidence-market fit because it has published a paper, completed a pilot, received positive user feedback or built a model.
A company has evidence-market fit when its evidence answers the question that the relevant decision-maker is actually asking.
The Odelle Evidence-Market Fit Framework
At Odelle Technology, we think evidence-market fit can be understood through seven linked elements:
Claim → Evidence → Comparator → Pathway → Economics → Implementation → Adoption
A company has evidence-market fit when these seven elements are aligned.
The claim must be precise enough to assess.
The evidence must support the claim being made.
The comparator must reflect real current practice.
The pathway must show where the technology changes a decision or outcome.
The economics must explain cost, value, budget impact or consequences.
The implementation plan must show that the technology can work in real settings.
The adoption route must match the market, payer, commissioner or procurement pathway.
If one of these elements is weak, the access story becomes fragile.
That fragility often appears late: after a pilot, after regulatory clearance, after investor funding, after launch preparation, or after a company enters a new country.
But the weakness usually begins much earlier.
It begins when evidence is generated without a clear view of the decision it must support.
Where evidence-market fit shows up in practice
Evidence-market fit is not theoretical. It appears repeatedly in the practical work companies need before reimbursement, procurement or adoption.
A diagnostic company may need to prioritise evidence because payer coverage is becoming more restrictive and clinical utility is not yet clear enough.
A medtech company may need a hospital-level budget impact model because clinical enthusiasm alone does not explain affordability to procurement committees.
An AI or digital health company may need to translate technical performance into workflow impact, safety, professional oversight and economic value.
An investor may need European reimbursement due diligence because a technology that looks attractive in one market may face very different coding, pricing, HTA and procurement barriers in France, Germany, Belgium, the Netherlands or the UK.
A pre-launch company may need a payer value story before pivotal evidence generation, because the wrong endpoints can create a reimbursement problem years later.
In each case, the issue is not whether the technology is interesting.
The issue is whether the evidence is aligned with the market decision.
That is evidence-market fit.
| Evidence-market fit problem | What companies often have | What decision-makers need |
|---|---|---|
| Diagnostic adoption | Analytical performance | Clinical utility, pathway impact and economic value |
| Digital health adoption | Engagement or usability data | Outcomes, safety, implementation and budget impact |
| AI in healthcare | Accuracy, AUC or model validation | Bias, drift, explainability, actionability and governance |
| Medtech procurement | Clinical enthusiasm | Hospital budget impact and workflow consequences |
| Investor diligence | Product-market story | Reimbursement risk, evidence gaps and adoption route |
| EU market entry | CE mark or technical promise | Country-specific coding, HTA, pricing and procurement logic |
The six layers of evidence-market fit
Evidence-market fit is not a single document.
It is an architecture.
At Odelle Technology, we see six layers.
1. Technical validity
Does the technology work as intended?
For a digital health tool, this may include software reliability, cybersecurity, interoperability, data quality, algorithm performance and usability.
For an AI system, it includes training data, validation data, model performance, subgroup performance, drift monitoring and transparency around limitations.
Technical validity is necessary.
But it is not enough.
A technology can work technically and still fail commercially if it does not change a meaningful decision.
2. Clinical or care validity
Does the technology measure, detect, predict, support or influence something that matters in a real clinical or care context?
For a diagnostic, this may mean sensitivity, specificity, positive predictive value and negative predictive value in the intended population.
For a digital care tool, it may mean identifying falls risk, medication non-adherence, deterioration or unmet support needs in a way that is reliable enough to act on.
This is where companies must be careful.
The intended use must be precise.
The evidence must support that intended use.
Broad claims create broad uncertainty.
3. Clinical or care utility
Does the technology change what happens next?
This is often the missing layer.
It is not enough to generate information. The information must change a decision, action, escalation, treatment, care plan or behaviour.
Does it reduce avoidable admissions?
Does it accelerate diagnosis?
Does it prevent deterioration?
Does it improve adherence?
Does it reduce unnecessary appointments?
Does it support earlier intervention?
Does it improve independence?
Does it reduce risk?
Clinical or care utility is where technology becomes pathway value.
4. Economic value
Does the technology create a credible economic argument?
This does not always mean full cost-effectiveness modelling. In many healthtech, medtech and digital care settings, a cost-consequence analysis or budget impact model may be more appropriate at the early stage.
But the economic logic must be explicit.
What costs are added?
What costs may be avoided?
Whose budget is affected?
Is staff time saved, shifted or increased?
Are admissions avoided?
Are complications reduced?
Are care packages delayed, reduced or stabilised?
Are implementation costs included?
Are training, support, maintenance and integration costs realistic?
This matters because digital and AI-enabled interventions often have complex cost structures. Their value may depend on adoption level, workflow integration, staff behaviour, data infrastructure, maintenance, upgrades, training and continued user engagement.
A digital technology is not just a product. It is often a service, workflow change and implementation programme at the same time.
5. Implementation validity
This may be the most underestimated layer.
Implementation validity asks whether a technology can work safely, consistently and affordably in real-world settings.
A technology may succeed in a pilot because the team is motivated, the supplier is closely involved and the patient population is carefully selected. That is not the same as working across routine NHS, local authority, care home, hospital or domiciliary care environments.
Implementation validity asks:
Can staff use it?
Does it fit workflow?
Does it integrate with records?
Are alerts actionable?
Who responds?
What happens at weekends?
What happens when staff are stretched?
Does it increase workload?
Does it shift work to unpaid carers?
Does it widen inequalities?
Can it be governed safely?
Can it scale without losing effectiveness?
This is where many digital health and AI companies underestimate the real access problem.
The question is not simply whether the technology works.
The question is whether it works inside the system expected to adopt it.
6. Trust and adoption confidence
The final layer is confidence.
Decision-makers need confidence before they fund, procure or scale a technology.
That confidence may come from independent evaluation, transparent methods, relevant comparators, credible endpoints, patient and carer involvement, professional acceptance, economic modelling, governance, certification and real-world implementation data.
This is where the UK and France are converging in different ways.
The UK is building confidence through NICE evidence standards and aligned access pathways.
France is building trust through HAS evaluation, professional-use guidance, certification and AI governance.
Both are asking the same underlying question:
Can this technology be trusted in the real system?
AI makes evidence-market fit harder, not easier
AI has made the evidence-market fit problem more urgent.
Many AI companies focus heavily on technical performance: accuracy, AUC, sensitivity, specificity, model validation and benchmark comparison.
Those metrics matter.
But they are not sufficient for adoption.
Health systems will ask harder questions.
Is the model safe across subgroups?
Does performance drift over time?
Who is accountable when the AI output is wrong?
How is the result explained to clinicians or patients?
Does the AI change a decision?
Can professionals override it?
Does it increase workload?
Does it create alert fatigue?
Does it introduce bias?
Does it require new governance?
Does it fit existing clinical or care pathways?
Does it improve outcomes, or only predictions?
This is why AI companies often need more than technical validation.
They need implementation validity, economic logic, governance evidence and adoption confidence.
For AI, evidence-market fit means proving not only that the model performs, but that the system can safely act on it.
The investor lesson: evidence-market fit is a valuation issue
Investors often ask whether a company has product-market fit.
In healthtech, that is not enough.
The better diligence question is:
Does the company have evidence-market fit?
This is not only a reimbursement issue.
It is a valuation issue.
A company may have technical risk reduced but adoption risk unresolved.
It may have regulatory progress but payer uncertainty.
It may have pilots but no scalable evidence.
It may have users but no reimbursement pathway.
It may have clinical enthusiasm but no economic model.
It may have a strong product narrative but no clear answer to the decision-maker’s question.
That matters because access risk affects time to revenue, pricing confidence, commercial partnerships, country sequencing, investor confidence and exit value.
A company without evidence-market fit may be moving quickly towards an access barrier.
What companies should ask before they scale
Before a company enters a new market, launches a pilot or raises capital on the basis of adoption potential, it should ask:
Who is the decision-maker?
What decision must they make?
What evidence do they need?
What comparator will they use?
What patient, clinician or care population matters?
What pathway does the technology change?
What cost consequences will be believed?
What implementation burden will be inherited?
What uncertainty remains?
What evidence can be generated now to reduce that uncertainty?
These questions are not bureaucratic.
They are commercial.
They determine whether a technology can move from promise to payment.
The Odelle view
At Odelle Technology, we believe the next competitive advantage in healthtech will not come only from better products.
It will come from better evidence architecture.
The companies that succeed will be those that understand early which market they are trying to enter, which decision-maker they need to convince, which evidence standard applies, which economic argument is credible, and which real-world pathway their technology must fit.
The question is no longer simply:
Can we build it?
Or:
Can we sell it?
Or:
Can we get it approved?
The question is:
Can we prove enough, to the right decision-maker, in the right format, at the right time, to support adoption, reimbursement or scale?
That is evidence-market fit.
How Odelle Technology can help
Odelle Technology helps healthtech, medtech, diagnostic, AI and digital care companies test evidence-market fit before launch.
This includes:
- mapping decision-makers;
- identifying evidence gaps;
- defining the comparator;
- clarifying the clinical or care pathway;
- building the payer and commissioner value story;
- developing budget impact and cost-consequence models;
- assessing implementation burden;
- designing real-world evidence strategies;
- preparing HTA, procurement and reimbursement narratives;
- sequencing access routes across the UK and Europe.
The purpose is simple: to help companies understand what they must prove before they ask health systems to pay, procure, recommend or scale.
Conclusion: product-market fit gets attention; evidence-market fit gets adoption
Product-market fit gets attention.
Evidence-market fit gets adoption.
That is the new reality for healthtech, medtech, digital health, AI, diagnostics and digital care companies.
The UK’s MHRA–NICE aligned pathway, NICE’s digital health evidence standards, the new adult social care evidence framework, and France’s HAS trust framework all point in the same direction.
Health systems are not rejecting innovation.
They are demanding better proof before scale.
For companies, that is not a threat if they prepare early.
It is an opportunity to build evidence strategically, align with decision-makers sooner, reduce adoption uncertainty and enter markets with a stronger value proposition.
For investors, it is a better diligence lens.
For health systems, it is a route to more confident adoption.
And for Odelle Technology, it is the core access question every serious health technology company should be asking:
Do we have evidence-market fit?
Because in healthcare, the market does not buy innovation alone.
It buys evidence it can trust.
References and further reading
- National Institute for Health and Care Excellence. MHRA–NICE pathway opens for business – everything you need to know to get started. Published 1 April 2026.
https://www.nice.org.uk/news/blogs/mhra-nice-pathway-opens-for-business-everything-you-need-to-know-to-get-started - GOV.UK. Get medicines to NHS patients earlier via the MHRA–NICE aligned pathway. Published 2026.
https://www.gov.uk/government/publications/get-medicines-to-nhs-patients-earlier-via-the-mhra-nice-aligned-pathway/get-medicines-to-nhs-patients-earlier-via-the-mhra-nice-aligned-pathway - National Institute for Health and Care Excellence. Evidence standards framework for digital health technologies.
https://www.nice.org.uk/what-nice-does/digital-health/evidence-standards-framework-esf-for-digital-health-technologies - Department of Health and Social Care / GOV.UK Social Care Blog. Deborah Sturdy. Developing evidence standards for digital technologies in adult social care. Published 19 May 2026.
https://socialcare.blog.gov.uk/2026/05/19/developing-evidence-standards-for-digital-technologies-in-adult-social-care/ - National Institute for Health and Care Excellence. Our evidence standards framework for digital care technologies. Published 28 April 2026.
https://www.nice.org.uk/news/blogs/our-evidence-standards-framework-for-digital-care-technologies - Haute Autorité de Santé. Technologies numériques et systèmes d’IA à usage professionnel. Updated 3 March 2026.
https://www.has-sante.fr/jcms/p_3363066/fr/technologies-numeriques-et-systemes-d-ia-a-usage-professionnel - Commission Nationale de l’Informatique et des Libertés. Numérique en santé : la CNIL et la HAS s’engagent pour renforcer les bonnes pratiques. Published 11 March 2026.
https://www.cnil.fr/fr/numerique-en-sante-la-cnil-et-la-has-sengagent - Unsworth H, Dillon B, Collinson L, et al. The NICE Evidence Standards Framework for digital health and care technologies – Developing and maintaining an innovative evidence framework with global impact. Digital Health. 2021.
https://pmc.ncbi.nlm.nih.gov/articles/PMC8236783/ - Stern AD, Brönneke J, Debatin JF, et al. Advancing digital health applications: priorities for innovation in real-world evidence generation. The Lancet Digital Health. 2022.
https://pubmed.ncbi.nlm.nih.gov/35216754/ - Gomes M, Murray E, Raftery J. Economic evaluation of digital health interventions: methodological issues and recommendations for practice. PharmacoEconomics. 2022.
https://link.springer.com/article/10.1007/s40273-022-01130-0 - Duffy S, Lee TH, et al. Real-world implementation of digital health interventions: a review of barriers and facilitators. 2022.
https://pmc.ncbi.nlm.nih.gov/articles/PMC9508664/ - Van Kessel R, Srivastava D, Kyriopoulos I, et al. Digital health reimbursement strategies of 8 European countries and Israel: scoping review and policy mapping. JMIR. 2023.
https://pmc.ncbi.nlm.nih.gov/articles/PMC10576236/